Free C 08 B Georgia Template in PDF
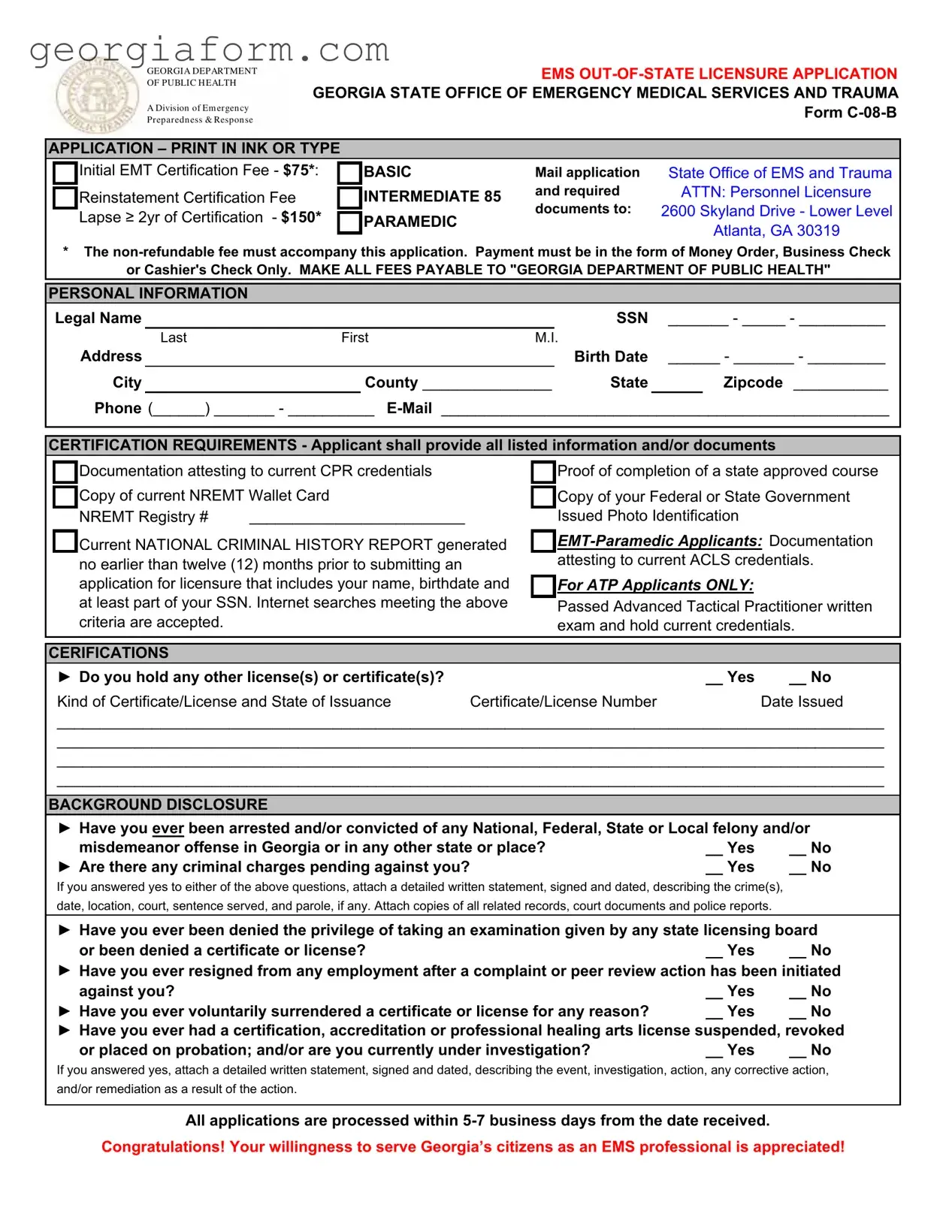
Individuals aspiring to serve as Emergency Medical Services (EMS) professionals in Georgia who are already licensed or certified in other states must navigate the required bureaucracy to ensure their qualifications are recognized within the state. The Form C-08-B, a document issued by the Georgia Department of Public Health’s Division of Emergency Preparedness & Response, is an essential part of this process. This out-of-state licensure application is designed for various levels of EMS professionals, including EMT-Basics, Intermediates, and Paramedics seeking initial certification, reinstatement, or renewal of their credentials in Georgia. Alongside personal information, applicants must provide proof of current CPR credentials, completion of a state-approved EMS course, a copy of their current National Registry of Emergency Medical Technicians (NREMT) wallet card, and a national criminal history report. In addition, paramedics are required to submit proof of Advanced Cardiac Life Support (ACLS) credentials, and Advanced Tactical Practitioner (ATP) applicants need to demonstrate that they have passed the relevant examination. The form mandates declarations regarding past criminal history, licensure denials, or any actions taken against an applicant's certification or license to ensure the integrity and proficiency of EMS providers. With a processing time of 5-7 business days from receipt, the thorough compilation of required documentation and the upfront disclosure of pertinent personal history underscore the comprehensive nature of the Form C-08-B, facilitating the smooth transition of EMS professionals into the state of Georgia’s emergency response framework.
Form Sample
GEORGIA DEPARTMENT OF PUBLIC H EALTH
A Division of Em er gen cy Pr epar edn ess & Respon se
EMS
APPLICATION – PRINT IN INK OR TYPE
|
Initial EMT Certification Fee - $75*: |
|
BASIC |
Mail application |
State Office of EMS and Trauma |
|
Reinstatement Certification Fee |
|
INTERMEDIATE 85 |
and required |
ATTN: Personnel Licensure |
|
|
||||
|
|
documents to: |
2600 Skyland Drive - Lower Level |
||
|
Lapse ≥ 2yr of Certification - $150* |
|
PARAMEDIC |
||
|
|
||||
|
|
|
Atlanta, GA 30319 |
||
|
|
|
|
|
* The
or Cashier's Check Only. MAKE ALL FEES PAYABLE TO "GEORGIA DEPARTMENT OF PUBLIC HEALTH"
PERSONAL INFORMATION
Legal Name |
|
|
|
|
|
SSN _______ - _____ - __________ |
||
|
Last |
First |
M.I. |
|
|
|
||
Address |
|
|
|
|
|
Birth Date |
______ - _______ - _________ |
|
City |
|
|
County _______________ |
State |
|
Zipcode ___________ |
||
Phone (______) _______ - __________
CERTIFICATION REQUIREMENTS - Applicant shall provide all listed information and/or documents
|
|
Documentation attesting to current CPR credentials |
|
|
Proof of completion of a state approved course |
||
|
|
Copy of current NREMT Wallet Card |
|
|
Copy of your Federal or State Government |
||
|
|
|
|
||||
|
|
NREMT Registry # |
_________________________ |
|
|
Issued Photo Identification |
|
|
|
Current NATIONAL CRIMINAL HISTORY REPORT generated |
|
||||
|
|
|
|||||
|
|
no earlier than twelve (12) months prior to submitting an |
|
|
attesting to current ACLS credentials. |
||
|
|
|
|
|
|
||
|
|
application for licensure that includes your name, birthdate and |
|
For ATP Applicants ONLY: |
|
||
|
|
at least part of your SSN. Internet searches meeting the above |
|
Passed Advanced Tactical Practitioner written |
|||
|
|
|
|
|
|
||
|
|
criteria are accepted. |
|
|
|
exam and hold current credentials. |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
CERIFICATIONS |
|
|
|
|
|
||
|
► Do you hold any other license(s) or certificate(s)? |
|
|
__ Yes |
__ No |
||
|
Kind of Certificate/License and State of Issuance |
Certificate/License Number |
Date Issued |
||||
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
BACKGROUND DISCLOSURE
► Have you ever been arrested and/or convicted of any National, Federal, State or Local felony and/or
misdemeanor offense in Georgia or in any other state or place? |
__ Yes |
__ No |
► Are there any criminal charges pending against you? |
__ Yes |
__ No |
If you answered yes to either of the above questions, attach a detailed written statement, signed and dated, describing the crime(s), date, location, court, sentence served, and parole, if any. Attach copies of all related records, court documents and police reports.
► Have you ever been denied the privilege of taking an examination given by any state licensing board
or been denied a certificate or license?__ Yes __ No ► Have you ever resigned from any employment after a complaint or peer review action has been initiated
against you? |
__ Yes |
__ No |
► Have you ever voluntarily surrendered a certificate or license for any reason? |
__ Yes |
__ No |
► Have you ever had a certification, accreditation or professional healing arts license suspended, revoked
or placed on probation; and/or are you currently under investigation?__ Yes __ No
If you answered yes, attach a detailed written statement, signed and dated, describing the event, investigation, action, any corrective action, and/or remediation as a result of the action.
All applications are processed within

GEORGIA DEPARTMENT OF PUBLIC H EALTH
A Division of Em er gen cy Pr epar edn ess & Respon se
GEORGIA OFFICE OF EMERGENCY MEDICAL SERVICES AND TRAUMA
AFFIDAVIT OF APPLICANT
I acknowledge and state that I have read and answered all questions in compliance with this application. I acknowledge that it is my responsibility to read and become familiar with the Georgia Department of Public Health Rules and Regulations for Emergency Medical Services
I further state that by filing this application for a license in the State of Georgia, I hereby authorize and consent to have an investigation made as to my moral character, professional reputation and fitness for practice as an EMS provider. I agree to give any further information which may be required in reference to my past record. I understand that I will not receive a copy of the report or know its contents and I further understand that the content of the investigative report will be privileged, unless determined otherwise by the Board or Court Order.
I hereby release, discharge, and exonerate the Georgia Department of Public Health, its agents, representatives, and any person so furnishing information, from any and all liability of every nature and kind arise out of the furnishing or inspection of such documents, records or other information or the investigation made by the Georgia Department of Public Health. I authorize the Georgia Department of Public Health to release information, material, documents, orders of the like relating to me or to this application to any other agency of the State of Georgia, the licensing agency of any other State or Territory of the United States or Province of Canada, a law enforcement agency, a hospital, or other agencies determined by the Board.
This is to certify that the foregoing information is true and correct to the best of my knowledge. I understand that any person who shall give false or forged evidence of any kind to the Board may be prosecuted to the fullest extent allowed by law.
Signature of Applicant |
|
Date |
|
|
|
|
|
Name Of Applicant |
|
City |
State |
Being duly sworn, says that he/she is the person who executed this application for licensure as an EMS provider in the State of Georgia; and that all the statements herein contained are true in every respect and that the attached photo is a true photo of applicant.
Sworn to and subscribed before me this ______ day of ___________, 20_____.
____________________________________________________
Notary Public
My Commission Expires _______________________________
(SEAL)
Attach Photo Here
Notary: DO NOT notarize this section unless a passport photograph is attached.
FORM
GEORGIA DEPARTMENT OF PUBLIC H EALTH
A Division of Em er gen cy Pr epar edn ess & Respon se
GEORGIA OFFICE OF EMERGENCY MEDICAL SERVICES AND TRAUMA
LICENSE VERIFICATION FORM
This form is used to verify the good standing of EMT or paramedic license or certification applicants who are licensed or certified by another state. Please note that you must submit a separate form for each license and/or certification you hold. Your application cannot be processed without this form.
PART I: Completed by Applicant
Legal Name: _______________________________________________ SSN: ______ - ______ - __________
Current Address: ______________________________________________________________________________
______________________________________________________________________________
►I am requesting Georgia license based on the following current license(s) or certification(s):
___ in the state of __________________ AND by the National Registry of EMTs
Current certification(s) or license(s) in another state or issued by the National Registry of EMTs:
EMT - Basic Certificate |
# ______________ |
Expiration Date |
____________________ |
|
EMT - Intermediate Certificate |
# ______________ |
Expiration Date |
____________________ |
|
Paramedic Certificate |
# |
______________ |
Expiration Date |
____________________ |
Other (specify) ______________________________________ |
|
|
||
Certificate |
# |
______________ |
Expiration Date |
____________________ |
PART II: Completed by the State Certifying Agency
Please assist by verifying that this individual is currently certified and in good standing according to your certification policies.
A. Is the
policy? |
__ Yes |
__ No |
B. Has the above certification(s) or license(s) ever been revoked or suspended? |
__ Yes |
__ No |
If yes, please explain ______________________________________________________________________ |
||
__________________________________________________________________________________________
__________________________________________________________________________________________
C. |
Has the above listed individual ever been convicted of a felony? |
__ Yes |
__ No |
|
If yes, what was the offense? _______________________________________________________________ |
||
|
Date of conviction ______________________ Place of conviction ________________________________ |
||
D. |
Do you know of any reason licensure in Georgia should be denied? |
__ Yes |
__ No |
|
If yes, please explain ______________________________________________________________________ |
||
__________________________________________________________________________________________
Title: _________________________
State: _________________________
Date: _________________________
Application Documents
Application Complete
Government Photo ID
Course Completion
NREMT Card
CPR Credentials
Nat'l Criminal Background
Other Certifications
(ATP, ACLS, ETC)
Application Fee
Type: __ M/O __ C/C __ B/C
CH # ________________________
Date: ____/_____/20______
Amount Recv'd: $ _____________
Recv'd by: __________________
|
Certification Status |
Status: __ Approved __ Denied |
|
Date: |
____/_____/20______ |
License # |
___________________ |
Exp Date: |
____/_____/20______ |
Notes: ____________________________
___________________________________
___________________________________
File Overview
| Fact Name | Description |
|---|---|
| Document Title | Georgia Out-of-State Licensure Application (Form C-08-B) |
| Governing Body | Georgia Department of Public Health, Division of Emergency Preparedness & Response; Georgia State Office of Emergency Medical Services and Trauma |
| Application Fees | Initial EMT Certification Fee - $75, Intermediate - $85, Paramedic Lapse ≥ 2yr of Certification - $150. Only Money Order, Business Check, or Cashier's Check accepted, payable to "GEORGIA DEPARTMENT OF PUBLIC HEALTH". |
| Certification Requirements | Includes submission of current CPR credentials, proof of completion of a state approved course, a copy of the current NREMT wallet card and a National Criminal History Report, among others. |
| Documentation for Specialized Certifications | For EMT-Paramedic applicants, documentation demonstrating current ACLS credentials is required. ATP applicants must have passed the Advanced Tactical Practitioner written exam and hold current credentials. |
| Background Disclosure Requirements | Applicants must disclose any arrests/convictions of misdemeanors or felonies, pending criminal charges, prior certification denial, employment terminations after complaints, voluntary surrender of any certificate or license, and any past or current investigations or sanctions. |
| Processing Time | All applications are processed within 5-7 business days from the date received. |
| Governing Laws | Rules and Regulations for Emergency Medical Services 111-9-2 under Georgia Law. |
Guide to Using C 08 B Georgia
Filling out the C 08 B Georgia form is an essential step towards obtaining EMS licensure for individuals already certified outside of Georgia. This form is pivotal for those looking to serve within Georgia's emergency medical services, ensuring applicants meet the required standards of knowledge and practice. The process includes verifying credentials, background checks, and ensuring you have the proper certification. By following these instructions precisely, you'll submit a complete and accurate application.
- Ensure you have all necessary personal information and documents at hand. These include your Social Security Number, legal name, contact information, proof of current CPR credentials, a state-approved course completion document, a copy of your current National Registry of Emergency Medical Technicians (NREMT) wallet card, and a photo ID.
- Gather your certification requirement documents, such as your CPR credentials, proof of course completion, NREMT wallet card, photo identification, a national criminal history report, and additional certifications if applicable (e.g., ACLS for paramedic applicants).
- Prepare a money order, business check, or cashier's check for the application fee. Remember, the fee is non-refundable, and the amount depends on your certification level and the exact nature of your application (initial certification, reinstatement, or lapse in certification).
- On the form, write your full legal name, social security number, address, birth date, and contact information in the designated spaces. Provide your email address as well.
- Under "Certification Requirements," check the boxes corresponding to the documents you are including with your application. List any other licenses or certificates you hold in the required section.
- In the "Background Disclosure" section, answer all questions truthfully. If you answer yes to any, attach a detailed statement explaining the circumstances, along with any relevant documentation such as court documents or police reports.
- Read the affidavit at the bottom of the form carefully. By signing it, you attest to the accuracy of the information you've provided and agree to the terms stated.
- Attach a passport-size photograph of yourself in the designated area, ensuring it meets any specified requirements.
- Review all sections of your application to ensure completeness and accuracy. Incomplete or incorrect applications can result in delays or denial of licensure.
- Mail the completed form with all necessary attachments and your payment to the address provided on the form. Use a secure and trackable mail service to ensure your application arrives safely.
After submitting your application, processing takes approximately 5-7 business days. It's essential to wait patiently and prepare for any further steps, such as additional verification or an interview. Successfully completing this application is a significant first step towards contributing to Georgia's emergency medical services. Your dedication to this vital field is appreciated.
Obtain Clarifications on C 08 B Georgia
What is the C-08-B Georgia form used for?
The C-08-B Georgia form is an application utilized by individuals who are seeking licensure to practice as Emergency Medical Services (EMS) providers in Georgia but are currently or were previously licensed in another state. It is a part of the licensing process overseen by the Georgia Department of Public Health's Division of Emergency Preparedness & Response.
Who needs to fill out the C-08-B form?
EMS professionals such as EMTs, paramedics, and advanced tactical practitioners moving to Georgia or seeking to practice in Georgia with a license obtained outside of the state must fill out the C-08-B form. This form is a requirement for those needing initial EMT certification, reinstatement, or lapsing in certification of 2 years or more.
What are the fees associated with the C-08-B application?
The application fees vary depending on the type of licensure and situation. For initial EMT certification, the fee is $75. Reinstatement certification and lapse of certification for more than 2 years carry a fee of $85 and $150, respectively. These fees are non-refundable and must be paid via Money Order, Business Check, or Cashier's Check, made payable to the "Georgia Department of Public Health."
What documents are required to complete the C-08-B form?
Applicants must provide a range of documents along with their C-08-B application, including proof of current CPR credentials, completion of a state-approved EMS course, a copy of their current NREMT wallet card and government-issued photo ID, and a national criminal history report generated no earlier than twelve months prior to submitting the application. EMT-Paramedic applicants also need to show documentation for current ACLS credentials, and ATP applicants must have passed the Advanced Tactical Practitioner written exam and hold current credentials.
How should I submit the completed C-08-B application?
Completed applications should be mailed to the State Office of EMS and Trauma at 2600 Skyland Drive - Lower Level, Atlanta, GA 30319. Ensure that all required documents and the appropriate fee accompany the application.
What happens after I submit the form?
After submission, your application will be processed within 5-7 business days. This process includes validating your credentials and reviewing your criminal history, if applicable. You might be contacted for further information or clarification during this period.
Who do I contact if I have questions about completing the form?
For questions regarding the completion or submission of the C-08-B form, you should contact the Georgia Office of Emergency Medical Services and Trauma. While specific contact information is not provided on the form, you can visit the Georgia Department of Public Health's official website or call their main line for guidance on the appropriate department to contact.
Can I check the status of my application?
The form does not specify how to check the status of your application, but typically, you may contact the office you submitted your application to for an update. Keep in mind that processing takes 5-7 business days, so it's advisable to allow for this time frame before inquiring.
What should I do if I've been convicted of a felony?
If you have been convicted of a felony, you must disclose this information on the C-08-B application. You're required to attach a detailed, signed, and dated statement describing the crime, date, location, court, sentence served, and if any, parole. Copies of all related records, court documents, and police reports should also be attached. Failure to disclose such information can affect your licensure status.
Is there a way to expedite the application process?
The form and provided guidance do not indicate an expedited process for the C-08-B application. The standard processing time is 5-7 business days, and it's suggested to ensure that your application is complete and accurate to avoid any potential delays.
Common mistakes
Filling out the C-08-B Georgia form, which is crucial for individuals seeking EMS licensure in Georgia, often involves various errors due to its comprehensive requirements. Identifying common mistakes can guide applicants through a smoother application process. Here are nine frequent mistakes:
Not using ink or typing: The form explicitly requires that it be filled out in ink or by typing, ensuring legibility and permanence of the information provided.
Incorrect fee payment method: Applicants sometimes overlook that the fee must be paid via Money Order, Business Check, or Cashier's Check only, and personal checks or cash are not accepted.
Omitting the non-refundable fee: Each application must be accompanied by the appropriate fee, reflective of the certification level applied for, which is crucial for the processing of the application.
Incomplete personal information: Failing to provide complete and accurate personal information, including Social Security Number, address, and contact details, can delay the processing.
Failure to attach required documentation: Documentation such as proof of CPR credentials, completion of a state-approved course, and a current NREMT Wallet Card must be included.
Submitting outdated criminal history reports: The National Criminal History Report needs to be generated no earlier than twelve (12) months before submitting the application to meet the recency requirement.
Neglecting certification requirements for specific levels: EMT-Paramedic applicants must provide proof of ACLS credentials, and ATP applicants need to have passed the Advanced Tactical Practitioner written exam with current credentials.
Incorrectly answering background disclosure questions: Applicants must carefully answer all background disclosure questions and attach detailed statements and documentation for any affirmative responses.
Not properly acknowledging and signing the affidavit: The application requires a signed acknowledgement of having read and answered all questions honestly, including accepting the terms for investigation into the applicant's moral character and fitness for practice.
Recognizing and avoiding these mistakes can significantly enhance the likelihood of a successful licensure application process, allowing applicants to serve as EMS professionals in Georgia. Paying close attention to the requirements laid out in the application instructions is essential for a seamless submission.
Documents used along the form
The journey to becoming an EMS professional in Georgia involves more than just filling out the Form C-08-B. Whether you are applying for the first time, seeking reinstatement, or looking to validate out-of-state credentials, several other forms and documents play crucial roles in the application process. Understanding each document's purpose will streamline your path to licensure.
- National Registry of Emergency Medical Technicians (NREMT) Certification: Proof of NREMT certification is necessary for those applying for reciprocity or reinstatement of a lapsed certification. It validates national-level EMS knowledge and skills.
- Current CPR Certification: This document proves the applicant’s competency in performing cardiopulmonary resuscitation, a fundamental skill required for all EMS professionals.
- Advanced Cardiac Life Support (ACLS) Certification: For Paramedic applicants, presenting a current ACLS card shows proficiency in handling cardiac emergencies. This validation is essential for higher-level EMS licensure.
- Government-Issued Photo Identification: A state-issued driver’s license or passport helps verify the identity of the applicant. This step is standard procedure in confirming that the applicant matches the credentials provided.
- National Criminal History Report: A complete background check ensures that the applicant meets the moral character and professional fitness standards necessary for public trust positions.
- Proof of Education or Training: Documentation from a state-approved EMS educational program certifies that the applicant has completed the required coursework and practical training for their licensure level.
- Licensure Verification Form: If licensed in another state, applicants must submit this form completed by their current or previous state’s EMS licensing body. It confirms the good standing and validity of an out-of-state license.
- Continuing Education Records: While not always required with the initial application, maintaining and sometimes submitting records of completed EMS continuing education is necessary for license renewal or reinstatement, demonstrating ongoing competency in the field.
Securing these documents and completing the necessary forms are steps on the pathway to EMS licensure in Georgia. Each piece plays an integral part in showcasing the applicant’s qualifications, ensuring that only competent and qualified individuals are entrusted with the responsibility of caring for Georgia's citizens in emergency medical situations.
Similar forms
The National Registry of Emergency Medical Technicians (NREMT) Application Form is similar in its aim to certify or recertify individuals based on their qualifications and previous education in the emergency medical services field. Both forms require proof of completion of an approved educational program, current CPR credentials, and a national criminal history report.
State Medical License Application Forms from other states share similarities with the C 08 B Georgia form through their requirements for personal information, educational background verification, and background disclosure regarding any past criminal activities or professional disciplinary actions. Applications often require the same level of detail about past education, current certifications, and legal standing.
The Advanced Cardiac Life Support (ACLS) Certification Application relates closely because it, too, asks for evidence of specific medical training and competence, such as CPR credentials for EMT-Paramedic applicants, similar to how the C 08 B form requires proof of ACLS for more advanced practitioners.
Licensure Verification Forms for professionals moving between states or verifying their license status for employment are akin to the second part of the C 08 B form, which focuses on confirming the good standing of an applicant's EMT or paramedic certification in their previous state. This part of the process ensures that an individual holds valid and current certifications without any history of revocation or serious disciplinary actions.
The Criminal Background Check Authorization Form bears resemblance in its purpose to collect details on the applicant's legal standing and history. Though it is more narrowly focused than the broader application form, the section of the C 08 B regarding national criminal history reports necessitates a similar disclosure of past criminal activities, an essential step for evaluating the suitability of a candidate in a trust-sensitive profession.
Professional Certification Renewal Forms found in various fields also mirror the reinstatement aspect of the C 08 B form, particularly for individuals who have allowed their certification to lapse for more than 2 years and are seeking to reinstate their professional status. There's a shared emphasis on documenting continuous education or recertification prerequisites, such as course completion and maintaining up-to-date emergency care credentials.
The Application for Professional License After Disciplinary Action is akin to sections of the C 08 B form where applicants must disclose prior criminal or professional disciplinary actions. Both types of applications necessitate transparency about past events that might influence the applicant's eligibility for certification or licensure, including the outcomes of any investigations, the nature of the offense, and rehabilitative actions taken since.
Dos and Don'ts
When filling out the C 08 B Georgia form for EMS out-of-state licensure application, certain steps should be taken to ensure a smooth and error-free submission process. Here are some do's and don'ts to consider:
Do:
- Print neatly in ink or type your responses to ensure all information is legible and can be understood by the personnel at the State Office of EMS and Trauma.
- Include the non-refundable fee with your application in the form of Money Order, Business Check, or Cashier's Check, as specified, ensuring it is payable to "GEORGIA DEPARTMENT OF PUBLIC HEALTH."
- Provide all required documentation as listed, such as current CPR credentials, proof of completion of a state-approved course, and a current NATIONAL CRIMINAL HISTORY REPORT generated no earlier than twelve months before the application submission.
- Accurately disclose any past criminal history, if applicable, attaching all necessary detailed written statements, court documents, and police reports as requested on the form.
Don't:
- Use payment methods not specified by the form, such as personal checks or cash, to avoid delays or application rejection due to non-compliance with submission guidelines.
- Leave sections blank or provide incomplete information, especially regarding personal information, certification requirements, and background disclosure, as this can lead to processing delays or denial of certification.
- Fail to attach required documents, such as a current photo ID, proof of course completion, or the appropriate fees, since these are critical for the processing of your application.
- Ignore the instructions to attach additional information if you’ve answered "Yes" to any questions related to criminal history or licensure denial, suspension, or revocation in another state or territory.
Misconceptions
When dealing with the complexities of the C-08-B Georgia Out-of-State Licensure Application for emergency medical services (EMS) personnel, several misconceptions can arise. It is important to clarify these misunderstandings to streamline the application process.
- Misconception 1: The application fee is refundable if the application is not successful.
This is not the case; the application fee is non-refundable regardless of the application outcome.
- Misconception 2: Personal checks are accepted for the application fee.
Only money orders, business checks, or cashier's checks are accepted. Personal checks will not be processed.
- Misconception 3: The National Criminal History Report can be older than 12 months.
Applicants must provide a National Criminal History Report generated no earlier than twelve (12) months prior to submitting the application, ensuring the information is current and accurate.
- Misconception 4: Internet prints of the National Criminal History Report are not acceptable.
Internet-based searches that meet the specified criteria are accepted, offering flexibility in obtaining this document.
- Misconception 5: Only EMT-Paramedic applicants need to submit documentation of their credentials.
While EMT-Paramedic applicants must provide proof of current ACLS credentials, all applicants must supply documentation such as CPR credentials, completion of a state-approved course, and a copy of their current NREMT wallet card.
- Misconception 6: If you have charges pending, you do not need to disclose this information.
Applicants must disclose if they have ever been arrested and/or convicted of any offense or if there are any criminal charges pending against them, ensuring full transparency.
- Misconception 7: You can apply without a current license or certification from another state.
The form requires information and verification of licensure and/or certification from another state, emphasizing the importance of being currently licensed or certified.
- Misconception 8: The application process is lengthy and takes several weeks.
All applications are processed within 5-7 business days from the date received, highlighting the efficiency of the review process.
Understanding these key points can significantly reduce confusion and ensure that applicants provide all necessary documentation and meet all requirements for their licensure application to be processed efficiently.
Key takeaways
Filling out and using the C 08 B Georgia form, which is the Out-Of-State Licensure Application for the Georgia State Office of Emergency Medical Services and Trauma, requires attention to detail and adherence to specific instructions. Below are key takeaways to ensure the application process is handled accurately.
- The non-refundable application fee differs based on the type of certification being applied for, and adequate payment must accompany the application submission. Acceptable forms of payment include Money Order, Business Check, or Cashier’s Check, made payable to the "Georgia Department of Public Health".
- Applicants must provide comprehensive personal information, including Legal Name, Social Security Number, Contact Information, and Documentation of their current qualifications. This includes CPR credentials, evidence of course completion approved by the state, a copy of the current National Registry of Emergency Medical Technicians (NREMT) Wallet Card, and photo identification among others.
- Background Disclosure is a crucial section of the application, requiring honest disclosures regarding any arrests, convictions, or pending criminal charges. Applicants with a positive history are mandated to attach a detailed written statement, including copies of all related records, court documents, and police reports. The same thorough documentation is required for any professional disciplinary actions, license denials, suspensions, or investigations.
- The application process includes a verification of the applicant's license status by the State Certifying Agency or the agency that issued the current certification. This form, which is part of the application packet, verifies the good standing and current status of the applicant's EMT or Paramedic license or certification. Without this form, the application cannot be processed.
This form serves as a critical step for professionals who possess certification outside of Georgia but wish to serve within the state’s EMS system, indicating Georgia’s commitment to maintaining a high standard of emergency medical service providers through detailed vetting and background checks.
Popular PDF Forms
Georgia Workers' Compensation Forms - Facilitates a more streamlined workers' compensation claim review process by providing comprehensive wage details.
Sales Tax Certificate of Exemption Georgia Purchaser - Clarifies that the tax-free treatment does not extend to purchases that the purchaser may donate or otherwise use for non-resale purposes.
Georgia G-1003 - Guidance for utilizing the vendor code when completing the G-1003 form for income statement returns.