Free Georgia Dma 6 Template in PDF
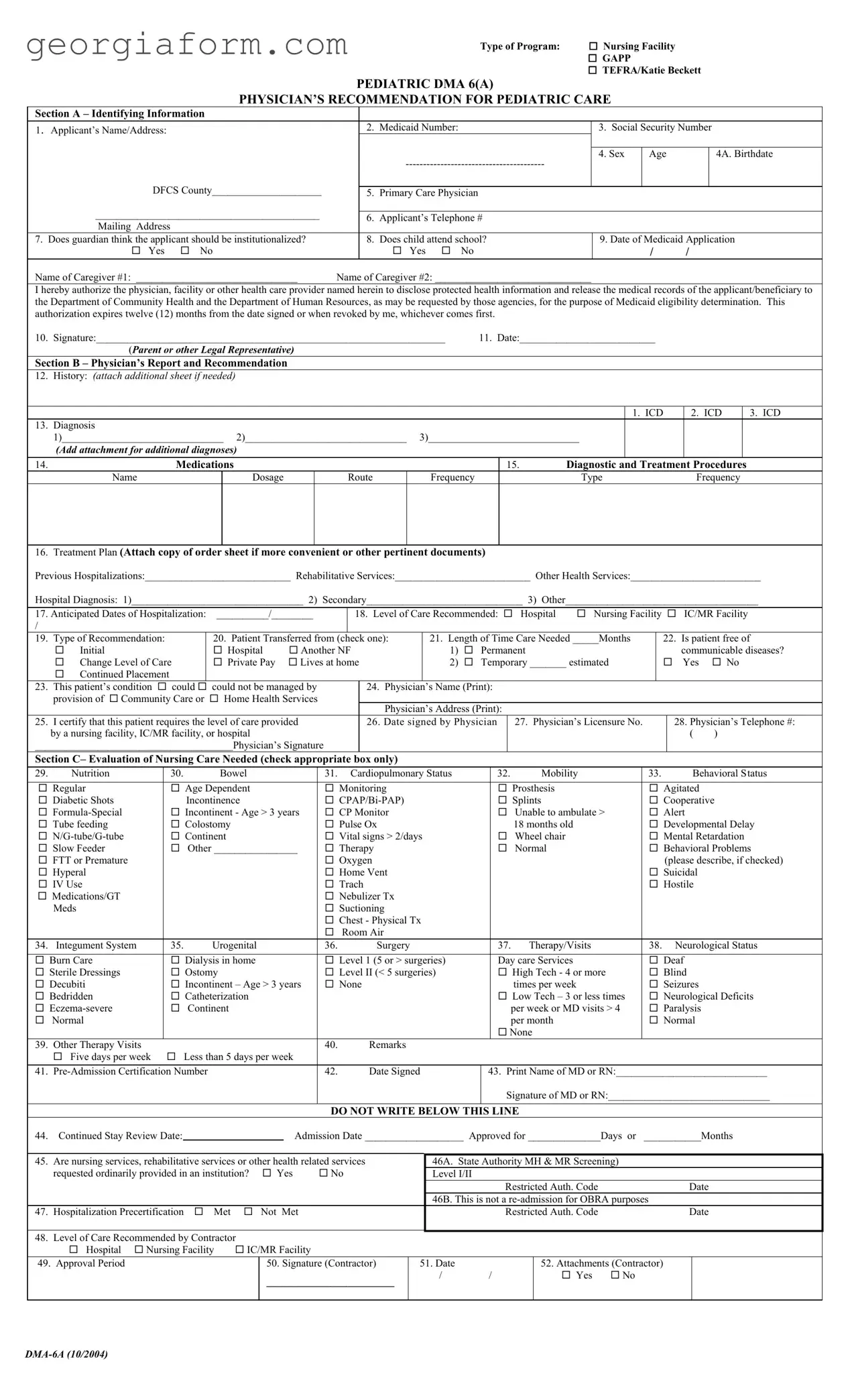
In the complex landscape of healthcare and medical eligibility, the Georgia DMA 6 form emerges as a crucial document for individuals seeking assistance within various programs, including Nursing Facility, GAPP, TEFRA/Katie Beckett, and particularly Pediatric care. This comprehensive form serves multiple purposes: it gathers identifying information about the applicant, such as name, Medicaid number, and social security number; it provides a channel for guardians to express their views on institutionalization; it traces the educational engagement of the child in question; and importantly, it facilitates a physician's detailed recommendation regarding the necessity of pediatric care. The form further includes sections for a physician's report on the applicant's medical history, diagnosis, treatment plan, and recommended level of care, alongside an evaluation of the nursing care needed. This meticulous compilation of data not only aids in the decisive process of Medicaid eligibility determination but also underlines the commitment of healthcare providers to tailor healthcare services to the nuanced needs of pediatric patients. By authorizing the release of medical records to the Department of Community Health and the Department of Human Resources, this form acts as a bridge between individual healthcare requirements and the administrative bodies tasked with the provision of essential services, thereby embodying a critical step in the journey towards healthcare access and management.
Form Sample
|
|
|
|
|
|
Type of Program: |
Nursing Facility |
|
|
|
|
|
|
|
|
|
|
GAPP |
|
|
|
|
|
|
|
|
|
|
TEFRA/Katie Beckett |
|||
|
|
|
PEDIATRIC DMA 6(A) |
|
|
|
|
|||
|
|
PHYSICIAN’S RECOMMENDATION FOR PEDIATRIC CARE |
|
|
|
|||||
Section A – Identifying Information |
|
|
|
|
|
|
|
|
||
1. |
Applicant’s Name/Address: |
|
|
2. |
Medicaid Number: |
|
3. Social Security Number |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Sex |
Age |
|
4A. Birthdate |
|
|
|
|
|
|
|
|
|
||
|
DFCS County_____________________ |
|
|
|
|
|
|
|
|
|
|
|
5. |
Primary Care Physician |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|||
|
___________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
6. |
Applicant’s Telephone # |
|
|
|
|
|||
|
Mailing Address |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
7. |
Does guardian think the applicant should be institutionalized? |
|
8. |
Does child attend school? |
9. Date of Medicaid Application |
|||||
|
Yes |
No |
|
|
Yes |
No |
|
/ |
/ |
|
Name of Caregiver #1: _______________________________ |
Name of Caregiver #2: ______________________________ |
|
|
|
|
|||||
I hereby authorize the physician, facility or other health care provider named herein to disclose protected health information and release the medical records of the applicant/beneficiary to the Department of Community Health and the Department of Human Resources, as may be requested by those agencies, for the purpose of Medicaid eligibility determination. This authorization expires twelve (12) months from the date signed or when revoked by me, whichever comes first.
10. Signature:___________________________________________________________________ |
11. Date:__________________________ |
(Parent or other Legal Representative) |
|
Section B – Physician’s Report and Recommendation
12. |
History: (ATTACH ADDITIONAL SHEET IF NEEDED) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. ICD |
|
|
2. ICD |
|
3. ICD |
||||
13. |
Diagnosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1)_______________________________ 2)_______________________________ 3)_____________________________ |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
(Add attachment for additional diagnoses) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
14. |
|
|
|
|
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. |
|
Diagnostic and Treatment Procedures |
||||||||||||||||||
|
|
Name |
|
|
|
|
|
|
|
Dosage |
|
|
|
Route |
|
|
Frequency |
|
|
|
|
|
|
Type |
|
|
|
Frequency |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
16. |
Treatment Plan (Attach copy of order sheet if more convenient or other pertinent documents) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
Previous Hospitalizations:____________________________ Rehabilitative Services:__________________________ Other Health Services:_________________________ |
||||||||||||||||||||||||||||||||||||||||
|
Hospital Diagnosis: 1)_________________________________ 2) Secondary______________________________ 3) Other_____________________________________ |
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
17. Anticipated Dates of Hospitalization: |
__________/________ |
|
|
|
18. |
Level of Care Recommended: |
Hospital |
Nursing Facility |
|
|
IC/MR Facility |
|||||||||||||||||||||||||||||
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. |
Type of Recommendation: |
|
|
|
20. Patient Transferred from (check one): |
|
21. Length of Time Care Needed _____Months |
|
22. Is patient free of |
||||||||||||||||||||||||||||||||
|
|
Initial |
|
|
|
|
|
|
|
Hospital |
|
Another NF |
|
|
|
1) |
Permanent |
|
|
|
|
|
|
|
communicable diseases? |
||||||||||||||||
|
|
Change Level of Care |
|
|
|
Private Pay |
|
Lives at home |
|
|
|
2) |
Temporary _______ estimated |
|
|
Yes |
|
No |
|||||||||||||||||||||||
|
|
Continued Placement |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
23. |
This patient’s condition |
could |
could not be managed by |
|
|
24. Physician’s Name (Print): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
provision of |
Community Care or |
|
Home Health Services |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician’s Address (Print): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
25. |
I certify that this patient requires the level of care provided |
|
|
26. Date signed by Physician |
|
27. |
|
Physician’s Licensure No. |
|
28. Physician’s Telephone #: |
|||||||||||||||||||||||||||||||
|
by a nursing facility, IC/MR facility, or hospital |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|||||||||||||
|
______________________________________Physician’s Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Section C– Evaluation of Nursing Care Needed (check appropriate box only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
29. |
Nutrition |
|
|
|
30. |
|
|
Bowel |
|
|
|
|
|
|
31. Cardiopulmonary Status |
|
32. |
|
|
Mobility |
|
33. |
|
|
|
Behavioral Status |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Regular |
|
|
|
|
Age Dependent |
|
|
|
|
Monitoring |
|
|
|
|
|
|
Prosthesis |
|
|
|
|
Agitated |
|
|
|
||||||||||||||
|
|
Diabetic Shots |
|
|
|
|
Incontinence |
|
|
|
|
|
|
|
|
|
|
|
|
Splints |
|
|
|
|
Cooperative |
|
|
||||||||||||||
|
|
|
|
|
Incontinent - Age > 3 years |
|
CP Monitor |
|
|
|
|
|
|
Unable to ambulate > |
|
Alert |
|
|
|
||||||||||||||||||||||
|
|
Tube feeding |
|
|
|
|
Colostomy |
|
|
|
|
|
|
Pulse Ox |
|
|
|
|
|
|
18 months old |
|
|
|
|
Developmental Delay |
|||||||||||||||
|
|
|
|
|
Continent |
|
|
|
|
|
|
Vital signs > 2/days |
|
|
|
|
Wheel chair |
|
|
|
|
Mental Retardation |
|||||||||||||||||||
|
|
Slow Feeder |
|
|
|
|
Other ________________ |
|
Therapy |
|
|
|
|
|
|
Normal |
|
|
|
|
Behavioral Problems |
||||||||||||||||||||
|
|
FTT or Premature |
|
|
|
|
|
|
|
|
|
|
|
|
|
Oxygen |
|
|
|
|
|
|
|
|
|
|
|
|
|
(please describe, if checked) |
|||||||||||
|
|
Hyperal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Vent |
|
|
|
|
|
|
|
|
|
|
|
|
|
Suicidal |
|
|
|
|||||||
|
|
IV Use |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trach |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hostile |
|
|
|
|||||
|
|
Medications/GT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nebulizer Tx |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Meds |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suctioning |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chest - Physical Tx |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Room Air |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
34. |
Integument System |
|
|
35. |
|
|
Urogenital |
|
|
|
|
36. |
|
|
Surgery |
|
|
|
37. |
|
Therapy/Visits |
|
38. |
|
Neurological Status |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Burn Care |
|
|
|
|
Dialysis in home |
|
|
|
|
Level 1 (5 or > surgeries) |
|
Day care Services |
|
|
|
|
Deaf |
|
|
|
||||||||||||||||||||
|
Sterile Dressings |
|
|
|
|
Ostomy |
|
|
|
|
|
|
Level II (< 5 surgeries) |
|
|
|
|
High Tech - 4 or more |
|
Blind |
|
|
|
||||||||||||||||||
|
Decubiti |
|
|
|
|
Incontinent – Age > 3 years |
|
None |
|
|
|
|
|
|
|
|
times per week |
|
|
|
|
Seizures |
|
|
|
||||||||||||||||
|
Bedridden |
|
|
|
|
Catheterization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low Tech – 3 or less times |
|
Neurological Deficits |
|||||||||||||||||
|
|
|
|
|
Continent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
per week or MD visits > 4 |
|
Paralysis |
|
|
|
||||||||||||||
|
|
Normal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
per month |
|
|
|
|
Normal |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
None |
|
|
|
|
|
|
|
|
|
|
|
|||
39. |
Other Therapy Visits |
|
|
|
|
|
|
|
|
|
|
|
|
|
40. |
|
|
Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Five days per week |
|
Less than 5 days per week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
41. |
|
|
|
|
|
|
|
|
42. |
|
|
Date Signed |
43. Print Name of MD or RN:_____________________________ |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of MD or RN:_______________________________ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DO NOT WRITE BELOW THIS LINE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
44. |
Continued Stay Review Date: |
|
|
|
|
|
|
|
Admission Date ___________________ Approved for ______________Days or ___________Months |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. |
Are nursing services, rehabilitative services or other health related services |
|
|
|
46A. State Authority MH & MR Screening) |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
requested ordinarily provided in an institution? |
Yes |
No |
|
|
|
Level I/II |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Restricted Auth. Code |
|
|
Date |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
46B. This is not a |
|
|
|
|
|
|
|
|||||||||||
47. |
Hospitalization Precertification |
|
|
Met |
|
Not |
Met |
|
|
|
|
|
|
|
|
|
Restricted Auth. Code |
|
|
Date |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
48. |
Level of Care Recommended by Contractor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Hospital |
Nursing Facility |
IC/MR Facility |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
49. |
Approval Period |
|
|
|
|
|
|
|
|
50. Signature (Contractor) |
|
51. Date |
|
|
|
|
|
|
52. Attachments (Contractor) |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
________________ |
|
/ |
/ |
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
File Overview
| Fact Number | Description |
|---|---|
| 1 | The Georgia DMA 6 form is used for recommending pediatric care under several programs including Nursing Facility, GAPP, TEFRA/Katie Beckett, and PEDIATRIC. |
| 2 | Section A of the form collects the applicant's identifying information, which includes name, Medicaid number, Social Security number, sex, age, birthdate, and contact details. |
| 3 | Questions in the form address the applicant’s school attendance, opinion on institutionalization, and Medicaid application date, requiring Yes or No answers. |
| 4 | The form requires a physician's recommendation, which includes medical history, diagnosis, medications, and treatment plan including any rehabilitative or other health services. |
| 5 | The form facilitates the authorization for the release of medical records to the Department of Community Health and the Department of Human Resources for Medicaid eligibility determination. |
| 6 | Authorization given on the form is valid for twelve months from the date signed or until revoked by the patient/representative, whichever comes first. |
| 7 | Section C assesses the extent of nursing care needed across various parameters including nutrition, mobility, cardiopulmonary status, and more. |
| 8 | The form is part of the Medicaid eligibility process in Georgia, guiding the state's decision on providing pediatric care within certain facilities or community/home health services. |
| 9 | It includes a section for physician’s licensure number and contact details to authenticate the professional recommendation for the required care. |
| 10 | The form adheres to the governing laws and regulations set by the Georgia Department of Community Health and is updated as per legislative or policy requirements. |
Guide to Using Georgia Dma 6
Filling out the Georgia DMA 6 form is a critical step for individuals seeking to ensure that their pediatric care needs are accurately communicated and processed for Medicaid eligibility and services. This form, detailed and comprehensive, requires input related to the applicant's personal information, medical history, and the physician's recommendations regarding the level of care needed. Careful completion of this document ensures that all necessary information is provided to the Department of Community Health and the Department of Human Resources, facilitating a smoother eligibility determination process. Here’s a step-by-step guide to help you navigate the necessary sections and ensure the form is completed accurately.
- Start with Section A – Identifying Information. Fill in the applicant’s name, address, Medicaid number (if available), social security number, sex, age, and birthdate. Don’t forget to include the DFCS County.
- Enter the name and contact information of the Primary Care Physician.
- Provide the applicant’s telephone number and mailing address.
- Answer whether the guardian thinks the applicant should be institutionalized and if the child is attending school currently by marking 'Yes' or 'No'.
- Fill in the date of the Medicaid application.
- Write down the names of Caregiver #1 and Caregiver #2, if applicable.
- Sign and date the form as the parent or other legal representative to authorize the release of medical information.
- Proceed to Section B – Physician’s Report and Recommendation. Record the medical history and attach additional sheets if necessary, citing the ICD codes.
- Detail the diagnosis or diagnoses in the provided spaces, attaching extra sheets for any additional diagnoses.
- List all current medications, including their dosage, route, and frequency.
- Document all diagnostic and treatment procedures, including the type and frequency.
- Describe the anticipated treatment plan, previous hospitalizations, rehabilitative services, and other health services. Attach copies of order sheets or pertinent documents for clarity.
- Indicate the anticipated dates of hospitalization and recommended level of care.
- Specify the type of recommendation and if the patient is being transferred from another facility. If known, mention the length of time care is needed.
- Answer if the patient is free of communicable diseases, marking 'Yes' or 'No'.
- Confirm if the patient’s condition could be managed by the provision of community care or home health services.
- Fill out the physician’s name, address, signature, date signed, licensure number, and telephone number.
- In Section C – Evaluation of Nursing Care Needed, check the appropriate boxes that describe the patient’s needs in terms of nutrition, bowel management, cardiopulmonary status, mobility, behavioral status, integument system, urogenital needs, surgical history, therapy/visits, and neurological status.
- Provide any additional remarks necessary for a comprehensive evaluation of the patient's condition.
- Include the Pre-Admission Certification Number and the date signed. Print and have the MD or RN sign the form to verify the information.
Once completed, review the form for accuracy and completeness. It's essential to provide as much detail as possible to support the Medicaid application and ensure the child receives the appropriate level of care. After the submission, the form will be assessed by the relevant state authorities to determine the child’s eligibility and the level of care approved.
Obtain Clarifications on Georgia Dma 6
-
What is the Georgia DMA 6 form used for?
The Georgia DMA 6 form is a crucial document utilized by healthcare providers and individuals applying for specific Medicaid-sponsored programs in Georgia. It serves multiple purposes, including the recommendation for pediatric care under various categories such as Nursing Facility, GAPP (Georgia Pediatric Program), TEFRA/Katie Beckett, and Pediatric. This form helps in identifying the level of care needed by the applicant, encompassing sections like patient information, physician’s report and recommendation, and the evaluation of nursing care needed.
-
What information is required on the DMA 6 form?
Completing the DMA 6 form necessitates providing detailed information across its various sections. In Section A - Identifying Information, details such as the applicant’s name, address, Medicaid and social security numbers, primary care physician, and caregiver’s information are required. It further asks questions about school attendance and the opinion of the guardian on institutionalization. Section B demands a comprehensive physician’s report and recommendation, including medical history, diagnoses, medications, treatment plan, and the level of care recommended. Lastly, Section C evaluates the nursing care needed, focusing on nutrition, mobility, behavioral status, and more, ensuring a holistic view of the patient’s needs.
-
How is the physician's recommendation for pediatric care determined?
The physician’s recommendation for pediatric care, outlined in the DMA 6 form, is determined through an extensive assessment of the child's medical condition. The physician is required to provide detailed information regarding the child's diagnoses, past and current treatments, medications, and the overall treatment plan. The assessment also includes evaluations of the child’s nutrition, mobility, behavioral status, and other health services that might have been utilized. This thorough investigation helps in deciding the most suitable level of care, whether it's hospitalization, a nursing facility, or at-home care, tailored to the pediatric patient’s specific needs.
-
How long is the authorization on the DMA 6 form valid, and can it be revoked?
The authorization granted through the DMA 6 form, allowing for the release of medical records and protected health information to the Department of Community Health and the Department of Human Resources for Medicaid eligibility determination, remains valid for twelve months from the date it is signed. However, this authorization is not irreversible; it can be revoked at any time within that 12-month period by the individual who granted it. This provision ensures that the applicant or their legal representative maintains control over their personal health information while also facilitating the necessary review for Medicaid eligibility purposes.
Common mistakes
Filling out the Georgia DMA 6 form requires careful attention to details. However, mistakes can occur for various reasons. Here are some common errors made while completing this form:
- Applicant’s identifying information is often incomplete. This section must include the full name, Medicaid number, Social Security number, age, birthdate, sex, and contact details.
- Omitting the primary care physician's name can delay the processing of the application. It is crucial to provide this information for a comprehensive review.
- Guardians sometimes miss answering whether they believe the applicant should be institutionalized. This question helps determine the level of care needed.
- Forgetting to specify if the child attends school. This information aids in understanding the daily routines and necessary support for the applicant.
- Leaving the date of Medicaid application blank can cause delays. It is essential for establishing timelines and eligibility.
- Not attaching an additional sheet when more space is needed for the physician’s report and recommendation. Detailed medical history and diagnoses are necessary for a thorough assessment.
- The medications and treatment plan sections are often incomplete. Accurately describing the medications, including dosage, route, and frequency, along with a comprehensive treatment plan, is critical for evaluating care needs.
- Forgetting to detail previous hospitalizations, rehabilitative services, and other health services. This information provides insight into the applicant's medical history and ongoing care requirements.
- Overlooking the necessity to check the level of care recommended and the type of recommendation. These sections are vital for ensuring the applicant receives appropriate support.
- Missing signatures and dates. The form requires signatures from the legal representative and the physician, along with the corresponding dates. These are legal attestations to the accuracy of the information provided.
Addressing these common errors can streamline the process of completing the Georgia DMA 6 form. Ensuring the form is filled out comprehensively and accurately is imperative for the timely and efficient processing of care requests.
Documents used along the form
When handling the Georgia DMA 6 form, which is essential for recommending pediatric care or institutional care, there are several other documents and forms that are often needed to support the application process. These additional materials play a crucial role in ensuring that the application is comprehensive, providing a thorough understanding of the applicant's needs and circumstances.
- Medical Records Release Form: This document is critical as it authorizes the release of the patient's medical records to the Department of Community Health and the Department of Human Resources. It ensures that the patient's medical history and current condition are accurately represented during the eligibility determination process.
- Proof of Legal Guardianship: If the person signing the DMA 6 form is not the parent of the child, a document proving legal guardianship or legal representation must be provided. This confirms the authority of the signatory to make medical and other important decisions on behalf of the applicant.
- ICD Diagnosis Codes Sheet: Since the DMA 6 form requires detailed information about the applicant's diagnoses, including ICD codes, an additional sheet listing all relevant diagnoses and their corresponding ICD codes can be necessary. This aids in providing a clear and detailed medical assessment for eligibility determination.
- Medication List: Similar to the diagnoses sheet, a comprehensive list of the applicant's medications—including dosages, frequency, and route of administration—is often required. This list gives a more complete picture of the patient's current treatment regimen.
- Treatment Plan: Although the DMA 6 form asks for treatment plans to be attached, providing a detailed and updated treatment plan document can further support the application. This plan should outline expected outcomes, anticipated services, and any rehab or specialized services the applicant is receiving or needs.
Together, these documents complement the Georgia DMA 6 form, creating a full picture of the applicant's healthcare needs and circumstances. By assembling all necessary forms and documents, applicants and their guardians can facilitate a smoother review process, aiming for a positive outcome in the Medicaid eligibility determination.
Similar forms
Medicare/Medicaid provider enrollment applications: These forms are used by healthcare providers to apply for the ability to participate in the Medicare or Medicaid programs. Similar to the Georgia DMA 6 form, which involves a physician's recommendation for pediatric care, these provider enrollment applications require detailed information about the healthcare provider's qualifications, services offered, and compliance with health program standards. Both types of documents are integral to securing healthcare services coverage under government programs.
Physician Certification for Durable Medical Equipment (DME): This document is necessary when a patient needs durable medical equipment, like wheelchairs or hospital beds, for use at home. Much like the DMA 6 form, it must be filled out by a physician or a qualified healthcare provider, outlining the medical necessity of the equipment for the patient’s condition. Both documents serve as critical validations for the need and appropriateness of specific healthcare services or equipment.
Disability determination forms: Employed by social security programs, these forms evaluate an individual's work limitations due to physical or mental conditions. They require detailed medical information about the individual's health status, similarly to the Georgia DMA 6 form, which involves assessments of the patient’s condition to determine the level of care needed. Both play key roles in accessing benefits tailored to individuals with specific health conditions.
Pre-authorization forms for treatment or procedures: These are required by health insurance companies before certain treatments, procedures, or medications are approved for coverage. They share similarities with the DMA 6 form in that a healthcare provider must supply detailed medical information and justification for the recommended service, ensuring it is necessary and appropriate for the patient's condition. Both types of documents facilitate the oversight and management of healthcare delivery.
Home health care certification and plan of care (Form CMS-485): Used in Medicare, this form is completed by a physician to certify that a patient needs home health services due to their medical condition. It outlines the types of services required, such as nursing care or physical therapy, mirroring the DMA 6 form’s function in recommending specific levels and types of pediatric care based on a thorough medical assessment. Both documents are vital for structuring patient-centered care plans within their respective care settings.
Dos and Don'ts
When filling out the Georgia DMA 6 form, specifically designed for physicians’ recommendations for pediatric care, attention to detail and understanding the form’s requirements are crucial. Below are several do’s and don’ts to assist in completing this form accurately.
- Do ensure that all personal information in Section A, including the applicant's name, address, Medicaid number, and Social Security number, is filled out completely and accurately. This is vital for the identification and processing of the application.
- Do obtain the signature of the parent or legal representative where indicated, as this is mandatory for the submission process. The signature, alongside the date, authorizes the release of medical records necessary for Medicaid eligibility determination.
- Do attach additional sheets if needed when detailing the applicant's medical history and current diagnosis in Section B. Providing comprehensive information can aid in the accurate assessment of the required level of care.
- Do thoroughly complete the Physician’s Report and Recommendation, ensuring the treatment plan, medications, and diagnosis are clearly noted. This section is critical for determining the necessity and type of care the child requires.
- Do not leave the anticipatory dates of hospitalization blank. If hospital care is expected, specifying these dates helps in planning and authorization of services.
- Do not forget to check the correct boxes in Section C– Evaluation of Nursing Care Needed. This section assesses the specific care requirements of the patient, so accuracy is paramount.
- Do not overlook the physician’s signature and licensure number at the end of Section B. Without this, the form may be considered incomplete and could delay processing.
By following these guidelines, the process of completing the Georgia DMA 6 form can be more straightforward, ultimately aiding in the timely and accurate assessment of the pediatric care needed.
Misconceptions
The Georgia DMA-6 Form is an essential document within the realm of Medicaid and healthcare planning in Georgia, particularly for pediatric care, nursing facility admissions, and other specialized care scenarios. However, surrounding this form, there are numerous misconceptions that can lead to confusion. Here, we aim to clarify some of these misunderstandings:
- Misconception 1: The Georgia DMA-6 form is applicable for adults seeking Medicaid assistance.
- Misconception 2: Guardian consent is not necessary for the institutionalization question.
- Misconception 3: The form is only for nursing facility admissions.
- Misconception 4: The form does not cover school attendance for the child.
- Misconception 5: There is no provision for authorizing the release of medical records through this form.
- Misconception 6: The physician's recommendation does not consider community-based care alternatives.
This is incorrect. The DMA-6 form, specifically the DMA-6A variant, is designed for pediatric care, hence the emphasis on sections like "Pediatric Care Physician’s Recommendation." For adults, different forms and procedures are applicable based on the type of care and Medicaid services required.
Contrary to this belief, the form explicitly asks whether the guardian thinks the applicant should be institutionalized. This indicates that guardian consent and their opinion are crucial components of the application process, reflecting the importance of family or guardian input in care decisions.
While it does cater to those seeking entry into a nursing facility, the scope of the DMA-6 form extends to broader pediatric care programs such as GAPP and TEFRA/Katie Beckett, beyond just nursing facility admissions. It plays a vital role in various pediatric healthcare settings.
In the "Identifying Information" section, there is a clear inquiry about whether the child attends school, highlighting the integration of healthcare needs with educational attendance and how it might affect the child's healthcare plan.
The document directly addresses the authorization for physicians, facilities, or other healthcare providers to disclose protected health information for Medicaid eligibility purposes. This authorization is paramount for facilitating a comprehensive review by the necessary departments.
Section B of the form allows physicians to specify whether the patient's condition could be managed by community care or home health services, among other settings. This part of the form recognizes the spectrum of care levels and the potential for non-institutional care pathways.
Understanding the DMA-6 form and its correct use is vital for healthcare providers, guardians, and applicants navigating Georgia's Medicaid system. Clearing up these misconceptions helps in ensuring that the form is filled out accurately, facilitating the appropriate care and support for pediatric patients.
Key takeaways
Understanding the Georgia DMA 6 Form is crucial for those applying for pediatric care under specific programs. Here are key takeaways to ensure accurate completion and submission:
- The form includes various sections, such as Identifying Information, Physician’s Report and Recommendation, and Evaluation of Nursing Care Needed.
- It is used for applications to programs like Nursing Facility, GAPP, TEFRA/Katie Beckett, and for Pediatric care.
- Applicant’s identifying information, including Medicaid number and Social Security Number, must be filled out accurately.
- Questions regarding the applicant's schooling, guardian's opinion on institutionalization, and contact information require clear answers.
- A signature from a parent or legal representative is necessary to authorize the release of medical records for Medicaid eligibility determination.
- The Physician’s section demands detailed medical history, diagnosis (including ICD codes), medications, and treatment plans. Supporting documents should be attached as needed.
- The form assesses the patient’s condition thoroughly to determine if it can be managed by community care or home health services, including an evaluation of nutrition, mobility, behavioral status, and more.
- The physician must certify that the recommended level of care is required, stating the anticipated duration of care and if the condition is communicable.
Accurate and complete submission of the Georgia DMA 6 Form is essential for facilitating the Medicaid eligibility and care recommendation process. Physicians and legal representatives should carefully review all sections before submission to ensure all necessary information is provided.
Popular PDF Forms
How to Keep Your Nursing License Active - The invitation for applicants to familiarize themselves with relevant laws and rules is a reminder of the professional and legal framework governing their practice.
Unemployment Insurance Benefit Determination Letter Georgia - Designed to gather information from businesses operating within the state, this document helps the Georgia Department of Labor track employment and organizational changes.