Free Georgia Medicaid Application Template in PDF
Filling out the Georgia Medicaid Application form is a critical step for residents seeking healthcare assistance. The form is meticulously designed to ensure that every applicant, irrespective of race, color, sex, age, disability, religion, national origin, or political belief, is considered fairly. Applicants are asked to provide a wealth of information, including personal details, living arrangements, and whether they are applying for Medicaid for themselves or others in their household. The form also inquires about pregnancy, unpaid medical bills, current health insurance coverage, diagnoses of breast or cervical cancer, and detailed financial information. Importantly, it emphasizes the need for accuracy and honesty in reporting income and resources, as these factors play a significant role in determining eligibility for Medicaid. Additionally, the form outlines the requirements for cooperation with the Division of Child Support Services in obtaining medical support from an absent parent, underlining the state's right to require such support and the consequences of non-cooperation. Completing the form is the first step in accessing crucial medical services, and assistance is offered to those who might find the application process challenging. The Georgia Medicaid Application form is comprehensive, ensuring that the process is thorough in capturing the necessary information to determine eligibility for healthcare support.
Form Sample
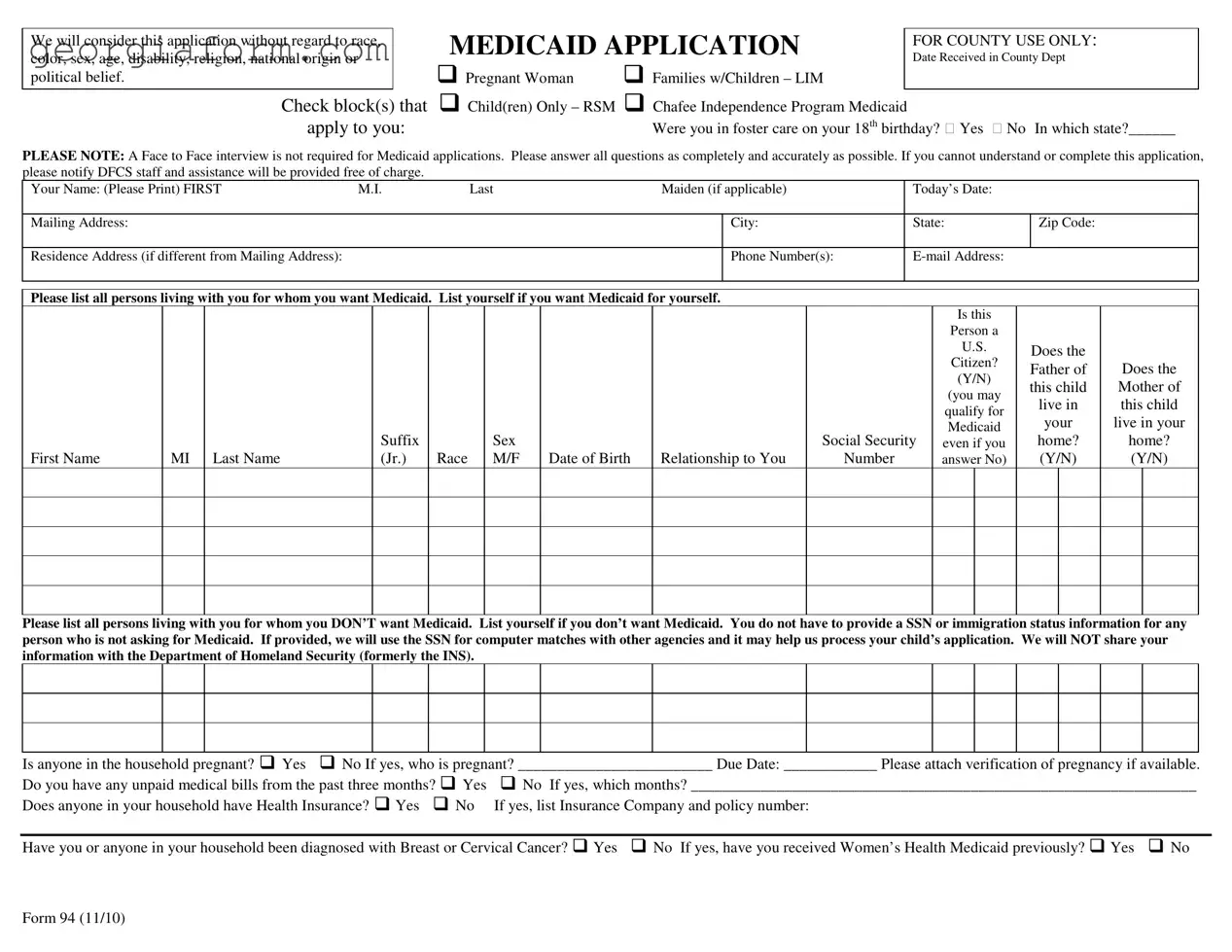
We will consider this application without regard to race, color, sex, age, disability, religion, national origin or political belief.
Check block(s) that apply to you:
MEDICAID APPLICATION |
FOR COUNTY USE ONLY: |
|
Date Received in County Dept |
||
|
Pregnant Woman Families w/Children – LIM
Child(ren) Only – RSM Chafee Independence Program Medicaid
Were you in foster care on your 18th birthday? Yes No In which state?______
PLEASE NOTE: A Face to Face interview is not required for Medicaid applications. Please answer all questions as completely and accurately as possible. If you cannot understand or complete this application, please notify DFCS staff and assistance will be provided free of charge.
Your Name: (Please Print) FIRST |
M.I. |
|
Last |
|
Maiden (if applicable) |
|
Today’s Date: |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address: |
|
|
|
|
|
|
|
|
|
City: |
|
State: |
|
Zip Code: |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Residence Address (if different from Mailing Address): |
|
|
|
|
|
|
|
Phone Number(s): |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Please list all persons living with you for whom you want Medicaid. List yourself if you want Medicaid for yourself. |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Is this |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Person a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U.S. |
|
Does the |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Citizen? |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Father of |
Does the |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
(Y/N) |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
this child |
Mother of |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
(you may |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
live in |
this child |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
qualify for |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
your |
live in your |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Medicaid |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Suffix |
|
|
Sex |
|
|
|
Social Security |
even if you |
|
home? |
home? |
||||
First Name |
MI |
Last Name |
|
(Jr.) |
Race |
|
M/F |
Date of Birth |
Relationship to You |
Number |
|
answer No) |
|
(Y/N) |
(Y/N) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please list all persons living with you for whom you DON’T want Medicaid. List yourself if you don’t want Medicaid. You do not have to provide a SSN or immigration status information for any person who is not asking for Medicaid. If provided, we will use the SSN for computer matches with other agencies and it may help us process your child’s application. We will NOT share your information with the Department of Homeland Security (formerly the INS).
Is anyone in the household pregnant? Yes No If yes, who is pregnant? _________________________ Due Date: ____________ Please attach verification of pregnancy if available.
Do you have any unpaid medical bills from the past three months? Yes |
No If yes, which months? _________________________________________________________________ |
Does anyone in your household have Health Insurance? Yes No |
If yes, list Insurance Company and policy number: |
Have you or anyone in your household been diagnosed with Breast or Cervical Cancer? Yes No If yes, have you received Women’s Health Medicaid previously? Yes No
Form 94 (11/10)
INCOME, RESOURCES and DAYCARE
List all income received by persons on page 1 of this application. Be sure to show the amount before deductions. Attach an extra sheet if necessary. We will decide, based on the type of Medicaid, whose income must be counted and whose may be excluded. If you are applying for Children Only or Pregnant Woman Medicaid, you do not have to complete the Resources/Vehicles sections below.
|
Gross Amount per Pay |
How Often? |
|
|
|
|
|
|
Amount in |
|
Who Owns |
||
|
Check |
(weekly, every |
|
|
|
|
|
|
|
||||
Income |
(amount before deductions) |
monthly, etc.?) |
Name of Person Receiving |
|
Resources |
|
Account/Value |
|
Resource? |
||||
Wages/Earnings |
|
|
|
|
Cash |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Current Employer: |
|
|
|
|
Checking Account |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Wages/Earnings |
|
|
|
|
Savings Account |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Current Employer: |
|
|
|
|
Credit Union |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Social Security |
|
|
|
|
401K/Retirement |
|
|
|
|
|
|
|
|
Income/SSI |
|
|
|
|
Account |
|
|
|
|
|
|
|
|
Worker’s |
|
|
|
|
|
|
|
|
|
|
|
|
|
Compensation |
|
|
|
|
Other |
|
|
|
|
|
|
|
|
Pensions or |
|
|
|
|
Vehicle(s): Cars, trucks, motorcycles (licensed) |
||||||||
Retirement Benefits |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Child Support/ |
|
|
|
|
Make |
|
Model |
|
Year |
|
Amount |
||
Contributions |
|
|
|
|
|
|
|
Owed? |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
Unemployment |
|
|
|
|
|
|
|
|
|
|
|
|
|
Benefits |
|
|
|
|
|
|
|
|
|
|
|
|
|
Other Income, please |
|
|
|
|
|
|
|
|
|
|
|
|
|
specify: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Do you pay for dependent care (daycare for a child or care for an adult who cannot care for himself/herself) so that someone in your household can work?
Name of Parent who works
Name of child or adult cared for
Name of care provider
Amount of Payment
How Often? (weekly,
monthly, etc)
If you are applying for Medicaid for children and one or both of their parents are not in the home, please provide the following information:
Child’s Name
Absent Parent’s Name (Mother/Father)
Do they have Medical Coverage on the Child?
Yes/No
If Yes to Medical Coverage, please list name
of insurance company & group number
I understand that this information may need to be verified to determine eligibility. I understand wage and salary information supplied by the Georgia Department of Labor may be obtained to verify and determine eligibility for Medicaid. I agree to assign to the state all rights to medical support and third party support payments (hospital and medical benefits). I agree to give the State the right to require an absent parent provide medical insurance, if available. I understand I must get medical support from the absent parent if it is available and must cooperate with the Division of Child Support Services in obtaining this support. If I do not cooperate, I understand I may lose my Medicaid benefits, and only my children will receive benefits unless good cause is established. I understand that I must report changes in my income and circumstances within ten (10) days of becoming aware of the change.
I certify under penalty of perjury that I am a U.S. Citizen and/or lawfully present in the United States. If I am a parent or legal guardian, I certify that the applicant(s) is a U.S. Citizen
and/or lawfully present in the United States. I certify to the best of my knowledge and belief that the person(s) for whom I am applying for Medicaid is/are U.S. citizen(s) or are lawfully present in the United States. I further certify that all of the information provided on this application is true and correct to the best of my knowledge.
Signature (Required): ______________________________________________________________________________ |
Date: ______________________________ |
Form 94 (11/10)
File Overview
| Fact Name | Description |
|---|---|
| Non-Discriminatory Statement | The application form explicitly states that it will be considered without regard to race, color, sex, age, disability, religion, national origin, or political belief. |
| Application Sections | The form includes sections for personal information, details about household members who are applying for Medicaid, information on health insurance and medical history, income, resources, and daycare expenses. |
| Support and Cooperation Clause | Applicants must agree to assign to the state all rights to medical support and third-party payments and cooperate with the Division of Child Support Services to obtain support from an absent parent, if available. |
| Interview Requirement | A face-to-face interview is not required for Medicaid applications, simplifying the application process for prospective beneficiaries. |
| Certification and Penalty Clause | Applicants must certify under penalty of perjury that they are a U.S. Citizen or lawfully present in the United States where applicable, and ensure all provided information is true and correct. |
Guide to Using Georgia Medicaid Application
Filling out the Georgia Medicaid Application form is a crucial step in accessing healthcare benefits for individuals and families in need within the state. The process is designed to be straightforward, but attention to detail is essential to ensure that all the required information is accurately provided. This guide will walk you through each step of completing the application, from checking the applicable blocks to providing detailed income and resource information. Taking the time to carefully review and fill out the form can lead to a smooth application process.
- At the top of the form, check the block(s) that apply to you. The options include "Pregnant Woman," "Families w/Children – LIM," "Child(ren) Only – RSM," and "Chafee Independence Program Medicaid."
- Answer the questions about being in foster care on your 18th birthday, including the state if applicable.
- Print your full name, including first name, middle initial, last name, and maiden name if applicable, in the designated space.
- Fill in today’s date, your mailing address, city, state, and zip code. Provide your residence address as well if it’s different from your mailing address.
- Enter your phone number(s) and email address in the spaces provided.
- List all persons living with you for whom you want Medicaid, including yourself, if applicable. For each person, provide the requested details such as whether the person is a U.S. Citizen, their relationship to you, and Social Security Number.
- For those individuals living with you for whom you do not want Medicaid, list their information separately, as instructed on the form. Remember, you do not need to provide a Social Security Number or immigration status for them.
- Indicate if anyone in the household is pregnant, and if so, provide the name of the person and their due date. Attach verification of pregnancy if available.
- Answer whether you have any unpaid medical bills from the past three months. If yes, specify the months.
- Indicate if anyone in your household has health insurance, listing the insurance company and policy number if applicable.
- Answer whether you or anyone in your household has been diagnosed with Breast or Cervical Cancer, and if you have received Women’s Health Medicaid previously.
- Under the "INCOME, RESOURCES, and DAYCARE" section, list all income received by persons on page 1 of this application before deductions and provide details on resources and daycare expenses as requested.
- If applicable, provide information about dependent care including the name of the parent who works, name of child or adult cared for, name of care provider, amount of payment, and payment frequency.
- For children applying for Medicaid when one or both parents are not in the home, provide the information requested regarding absent parent(s) and their medical coverage for the child.
- Read the acknowledgments and agreements carefully regarding rights to medical support, requirement to report changes in income and circumstances, and certification of the truthfulness of your application. Then, sign and date the form where indicated.
After completing the form, review all the information to ensure accuracy and completeness. Submit the application to the designated county department as indicated on the form or as directed by local guidelines. The processing of your application will then begin, and you may be contacted for further information or clarification as needed. Accurate and complete applications help streamline the process, making it easier for both the applicant and the reviewing agency.
Obtain Clarifications on Georgia Medicaid Application
-
Who can apply for Georgia Medicaid?
Anyone living in Georgia who meets the eligibility criteria can apply for Medicaid. This includes pregnant women, families with children, and individuals who were in foster care on their 18th birthday. It's designed for those who have low income or specific medical needs.
-
Do I need to schedule an in-person interview to complete my Medicaid application?
No, a face-to-face interview is not required for Medicaid applications in Georgia. You can complete and submit your application without an in-person meeting.
-
What happens if I can't understand or complete the Medicaid application on my own?
If you're having trouble with the application, don't worry. Assistance is available free of charge. You should notify the staff at the Division of Family and Children Services (DFCS), and they will help you through the process.
-
Can I apply for Medicaid for other people living with me?
Yes, on the application, you can list all the people living with you who you want to receive Medicaid. Make sure to include their relationship to you, their citizenship status, and other necessary information as indicated on the form.
-
What information do I need to provide about household members not applying for Medicaid?
For individuals in your household who are not applying for Medicaid, their social security numbers and immigration status are not required. However, providing this information may assist in the processing of your application, if applicable.
-
What should I do if someone in my household is pregnant?
If someone in your household is pregnant, indicate this on your application and, if available, attach verification of the pregnancy. This information is important as pregnant women may be eligible for different benefits.
-
How do unpaid medical bills affect my Medicaid application?
When applying, disclosing any unpaid medical bills from the past three months is necessary. This information can potentially qualify you for coverage of these bills through Medicaid.
-
What income and asset information must be provided?
For your application, you'll need to list all income sources and their amounts before deductions for everyone applying. If you're applying for Children Only or Pregnant Woman Medicaid, you do not need to fill out the sections about resources/vehicles.
-
I have a child and the other parent is not living with us. What information do I need to provide?
If you're applying for Medicaid for children who have a parent not living in the household, you need to provide the name of the absent parent, indicate whether the child has medical coverage, and if so, list the insurance company and group number.
-
What are my responsibilities after filing the Medicaid application?
After applying, you must report any changes in your income or circumstances within ten days of becoming aware of the change. Cooperation in obtaining medical support from an absent parent is required unless good cause is established; otherwise, you may lose your benefits.
Common mistakes
- Not providing complete and accurate information for all household members. Many applicants fail to list every person living in the household or inaccurately report their income and expenses. This can lead to delays or denials in processing the Medicaid application.
- Overlooking the requirement to attach verification documents. Applicants sometimes forget to include essential documents such as proof of pregnancy or unpaid medical bills from the past three months. Without these verifications, the application cannot be fully processed.
- Incorrectly handling the sections about people not requesting Medicaid. Some people mistakenly provide Social Security numbers or immigration status information for household members who are not applying for Medicaid benefits. This is not required and can create confusion.
- Failing to report recent changes in income or circumstances within ten days. It’s crucial to keep Medicaid information up to date, but many applicants do not report changes in their financial situation or household structure in a timely manner.
- Misinterpreting the need for cooperation with the Division of Child Support Services. Applicants sometimes do not realize that in order to receive Medicaid benefits, they must cooperate in obtaining medical support from an absent parent if it's available. This oversight can result in individuals losing their Medicaid benefits.
Documents used along the form
Applying for Medicaid in Georgia involves more than just completing the application form itself. To accurately assess eligibility and ensure the provision of benefits, applicants are often required to provide additional documentation and forms that offer a comprehensive picture of their financial and personal situation. Below is a list of documents commonly required alongside the Georgia Medicaid Application form.
- Proof of Income: This includes documents such as pay stubs, tax returns, and social security income statements. These are essential for verifying the income listed on the Medicaid application, helping to determine the applicant's financial eligibility for Medicaid benefits.
- Proof of Citizenship or Legal Status: Applicants must provide documents such as birth certificates, passports, or immigration papers. This documentation is crucial for verifying the applicant's legal status in the United States, a requirement for Medicaid eligibility.
- Proof of Pregnancy: If applicable, documents such as a doctor's note or medical records proving pregnancy are necessary. This information is used to determine eligibility for Medicaid benefits that are specifically available to pregnant women.
- Identification Documents: This includes a government-issued photo ID, such as a driver's license or state ID card. Identification helps to verify the applicant's identity and prevent fraudulent applications.
- Proof of Residence: Documents such as utility bills, rental agreements, or mortgage statements are required to prove the applicant's residence in Georgia. This is essential for establishing that the applicant is indeed applying for Medicaid in the correct state and is a resident who qualifies for state-specific Medicaid benefits.
- Medical Bills or Expenses: Unpaid medical bills or receipts for medical expenses can also be necessary, particularly if the applicant is applying for Medicaid with the intention of covering past medical expenses. These documents can help to establish the need for medical assistance and potentially increase the urgency or level of benefits provided.
Completing the Medicaid application process accurately and thoroughly is crucial for individuals and families seeking medical assistance through Georgia's Medicaid program. By providing the necessary additional forms and documentation, applicants can help ensure that their eligibility is assessed correctly and that they receive any benefits for which they are eligible. Understanding the types of documents required can simplify the application process and help applicants to prepare more effectively.
Similar forms
The Federal Income Tax Return shares similarities with the Georgia Medicaid Application form in that both require detailed income information to assess eligibility for benefits or tax liability. The need to report all sources of income and certain expenses aligns closely with Medicaid's requirement to consider an applicant's financial state.
The Supplemental Nutrition Assistance Program (SNAP) Application is akin to the Medicaid form mainly in its assessment of household composition and income. Both determine eligibility based on the size of the household, income, and resources, ensuring that assistance is provided to those most in need.
Children’s Health Insurance Program (CHIP) Application mirrors the Medicaid Application due to its focus on providing health coverage to eligible children. It similarly asks detailed questions about the child’s living situation, parental information, and existing health coverage, emphasizing the importance of accurate family and financial information.
Free Application for Federal Student Aid (FAFSA) aligns with the Medicaid application by requiring personal and financial information to evaluate eligibility for assistance. Although FAFSA targets educational funding, both demand disclosures of income and assets to determine benefit qualification.
The Temporary Assistance for Needy Families (TANF) Application is also like the Medicaid form as it evaluates financial hardship and family composition to assist those in dire need. The focus on the family unit and the provision of necessary details about household members and their financial circumstances make these forms comparable.
Subsidized Housing Applications, such as those for Section 8, share similarities with the Medicaid Application because they both require applicants to provide thorough details on income, family size, and living situation to qualify for assistance, ensuring that help reaches the right individuals based on their needs and resources.
The Application for Social Security Benefits is similar to the Medicaid Application, albeit with a focus on retirement, disability, or survivor benefits. Both necessitate comprehensive personal, financial, and in some instances, health information, to establish eligibility for government-provided benefits.
Dos and Don'ts
Applying for Georgia Medicaid requires attention to detail and thoughtful consideration in order to ensure that the application process is smooth and the determination of eligibility is accurate. Below is a list outlining what you should and shouldn't do when filling out the Georgia Medicaid application form:
Do:- Provide complete and accurate information for all questions to the best of your ability. Incomplete or inaccurate information can delay the application process or lead to a denial of eligibility.
- Be prepared to attach necessary verifications, such as proof of pregnancy or unpaid medical bills from the past three months if applicable. This supports your application and may expedite processing.
- If you are unsure about any part of the application or cannot complete it on your own, seek assistance from DFCS staff. They are there to help you free of charge.
- Include information about all individuals living with you who need Medicaid, as well as those for whom you are not seeking Medicaid. This comprehensive household overview is crucial for an accurate assessment.
- List all sources of income before deductions, as your eligibility for Medicaid may be determined based on your household's total income.
- Avoid the presumption that a face-to-face interview is required for all applications. It is noted that a face-to-face interview is not mandatory for Medicaid applications in Georgia.
- Do not omit information about anyone living with you, whether or not you are applying for Medicaid for them. This full disclosure is essential for a correct eligibility determination.
- Fail to list the Social Security Number (SSN) for individuals applying for Medicaid. While you don't have to provide it for those who aren't applying, listing it where applicable can help expedite the process.
- Do not leave sections blank if they apply to you. For instance, if asking about children's medical coverage when a parent is not in the home, complete all relevant sections to provide clarity on your situation.
- Avoid misrepresentations or inaccuracies in your application. The certification at the end of the application, under penalty of perjury, underscores the importance of the accuracy of your information.
Understanding and following these directives can help ensure your Georgia Medicaid application is processed efficiently, leading to a quicker determination of your eligibility.
Misconceptions
When navigating the process of applying for Medicaid in Georgia, several misconceptions can create confusion and sometimes result in incorrect applications or forgone opportunities for assistance. Below, some of these misconceptions are clarified to aid individuals in their application process:
- Myth 1: All applicants are required to undergo a face-to-face interview. Contrary to popular belief, Georgia Medicaid applications do not mandate a face-to-face interview, aiming to streamline the process and make it more accessible for everyone, regardless of their ability to travel to an agency office.
- Myth 2: Providing social security numbers for all household members is mandatory, even if they are not applying for Medicaid. In reality, only those seeking Medicaid need to provide their social security numbers (SSN). Applicants are not obliged to disclose the SSNs of non-applicants in the household, minimizing privacy concerns.
- Myth 3: Information shared on the Medicaid application will be shared with the Department of Homeland Security (DHS). It's important to understand that the information provided for Medicaid, including SSNs, is not shared with DHS, reassuring applicants concerned about immigration status disclosures.
- Myth 4: Medicaid eligibility is influenced by race, religion, or political beliefs. The application process is impartial, with eligibility determined without regard to race, color, sex, age, disability, religion, national origin, or political belief, ensuring a fair assessment for all applicants.
- Myth 5: You must complete the resources and vehicles section, no matter what type of Medicaid you are applying for. This is not the case for everyone. Applicants for Children Only or Pregnant Woman Medicaid can bypass the sections on resources/vehicles, simplifying the process for those specific groups.
- Myth 6: If you are applying for your children and you are living with them, both parents must be living in the home for the children to qualify. Medicaid eligibility for children does not hinge on both parents living in the household. The application invites details on absent parents, indicating that single-parent households are also considered.
- Myth 7: Assistance for completing the application is not readily available. The Department of Family and Children Services (DFCS) explicitly offers help for anyone who struggles to understand or complete the application. This service is provided free of charge, ensuring applicants can accurately complete their applications with the necessary support.
Correcting these misconceptions ensures that individuals are well-informed about the process and requirements of the Georgia Medicaid Application, enabling them to pursue the support they need confidently and accurately.
Key takeaways
Filling out the Georgia Medicaid Application form accurately is crucial for ensuring you or your dependents receive the necessary healthcare coverage. Below are key takeaways to help you navigate the process smoothly:
- All applicants will be considered for Medicaid without regard to race, color, sex, age, disability, religion, national origin, or political belief, promoting an inclusive approach to healthcare access.
- Prospective applicants do not need to attend a face-to-face interview, simplifying the application process.
- It's important to answer all questions as completely and accurately as possible to avoid delays in the processing of the application.
- Assistance is available free of charge for those who find the application challenging to understand or complete, ensuring support is accessible to everyone.
- Applicants must list all persons living in the household for whom Medicaid is sought, as well as those for whom it is not, streamlining the eligibility determination process.
- The application asks for information on current health insurance, unpaid medical bills, and if anyone has been diagnosed with Breast or Cervical Cancer, which helps in tailoring the healthcare coverage.
- Income and resources of the household must be disclosed to determine eligibility, except when applying for Children Only or Pregnant Woman Medicaid where this information may not be necessary.
- Applicants must report changes in income and circumstances within ten days to maintain their eligibility status, highlighting the importance of ongoing communication.
- By signing the application, applicants certify under penalty of perjury their citizenship status and the accuracy of the information provided, emphasizing the seriousness of the application process.
- The form facilitates the assignment of rights to medical support and third-party payments to the state, ensuring that beneficiaries maximize all available resources for their healthcare needs.
Understanding these key aspects can greatly assist applicants in navigating the Georgia Medicaid Application process, facilitating a smoother and more efficient experience in securing healthcare coverage.
Popular PDF Forms
Georgia Workers' Compensation Forms - Outlined with designated spaces for typing or printing information, promoting legibility in submissions.
Work Comp Georgia - It is the employer's responsibility to accurately complete and timely submit the WC-3 form to contest a compensation claim effectively.