Free Georgia Wc 14 Template in PDF
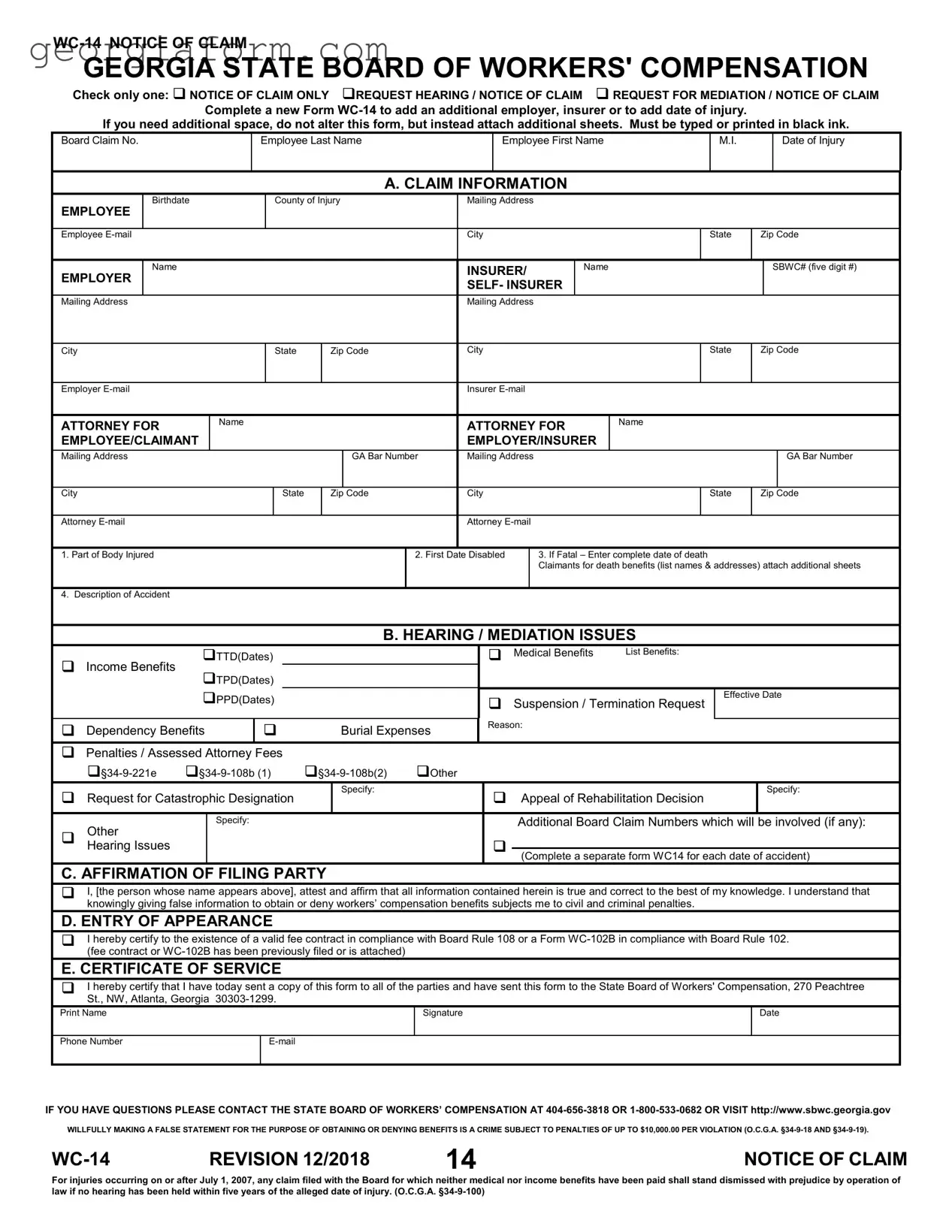
In the realm of workers' compensation in Georgia, navigating the claims process requires a thorough understanding of specific forms and procedures, among which the WC-14 Notice of Claim form stands as a cornerstone for initiating claims. This comprehensive document serves multiple crucial purposes: it can be utilized strictly as a notice of claim, a request for a hearing coupled with a notice of claim, or as a request for mediation in conjunction with a notice of claim. Designed to guide injured workers or their representatives through the process of formally notifying the Georgia State Board of Workers' Compensation about an injury or occupational illness, the form demands detailed information about the claimant, the employer, and the insurer or self-insurer involved, in addition to specifics about the injury, such as the body part affected, the first date of disability, and a descriptive account of the accident. Moreover, it addresses the need for a delineation of issues for which a hearing or mediation is sought, including but not limited to temporary or permanent disability benefits, medical benefits, and potential penalties or assessed attorneys' fees. The form further prompts the affirmation of the filing party regarding the truthfulness of the provided information, under penalty of civil and criminal repercussions for misconduct, and necessitates a certificate of service proving notification to relevant parties, thereby binding them into the adjudicative process. Thus, the WC-14 form embodies more than just a bureaucratic step; it encapsulates a critical pathway for employees to assert their rights to compensation and rehabilitation in the aftermath of work-related injuries or diseases.
Form Sample
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
Check only one: NOTICE OF CLAIM ONLY REQUEST HEARING / NOTICE OF CLAIM REQUEST FOR MEDIATION / NOTICE OF CLAIM
Complete a new Form
If you need additional space, do not alter this form, but instead attach additional sheets. Must be typed or printed in black ink.
Board Claim No.
Employee Last Name
Employee First Name
M.I.
Date of Injury
A. CLAIM INFORMATION
EMPLOYEE
Birthdate
County of Injury
Mailing Address
Employee
City
State
Zip Code
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
INSURER/ |
|
Name |
|
|
|
|
|
SBWC# (five digit #) |
||||
EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
SELF- INSURER |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
State |
Zip Code |
City |
|
|
|
|
|
|
State |
Zip Code |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Employer |
|
|
|
|
|
|
|
|
|
Insurer |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ATTORNEY FOR |
|
Name |
|
|
|
ATTORNEY FOR |
Name |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
EMPLOYEE/CLAIMANT |
|
|
|
|
|
|
|
|
|
EMPLOYER/INSURER |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Mailing Address |
|
|
|
|
|
|
|
GA Bar Number |
Mailing Address |
|
|
|
|
|
|
|
|
GA Bar Number |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City |
|
|
|
|
|
State |
Zip Code |
City |
|
|
|
|
|
|
State |
Zip Code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Attorney |
|
|
|
|
|
|
|
|
|
Attorney |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
1. Part of Body Injured |
|
|
|
|
|
|
|
|
2. First Date Disabled |
|
|
3. If Fatal – Enter complete date of death |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Claimants for death benefits (list names & addresses) attach additional sheets |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Description of Accident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
B. HEARING / MEDIATION ISSUES |
|
|
|
|
|
|||||||||
|
|
TTD(Dates) |
|
|
|
|
|
|
Medical Benefits |
List Benefits: |
|
|
|
|
|
||||||||
Income Benefits |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
TPD(Dates) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
PPD(Dates) |
|
|
|
|
Suspension / Termination Request |
|
Effective Date |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
Reason: |
|
|
|
|
|
|
|
|
|
||
Dependency Benefits |
|
|
Burial Expenses |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Penalties / Assessed Attorney Fees
|
Other |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Request for Catastrophic Designation |
|
Specify: |
|
|
Appeal of Rehabilitation Decision |
Specify: |
||
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Other |
|
Specify: |
|
|
|
|
Additional Board Claim Numbers which will be involved (if any): |
|
|
|
|
|
|
|
|
|
|
|
|
Hearing Issues |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Complete a separate form WC14 for each date of accident) |
|||
|
|
|
|
|
|
|
|||
C. AFFIRMATION OF FILING PARTY
I, [the person whose name appears above], attest and affirm that all information contained herein is true and correct to the best of my knowledge. I understand that knowingly giving false information to obtain or deny workers’ compensation benefits subjects me to civil and criminal penalties.
D. ENTRY OF APPEARANCE
I hereby certify to the existence of a valid fee contract in compliance with Board Rule 108 or a Form
E. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all of the parties and have sent this form to the State Board of Workers' Compensation, 270 Peachtree St., NW, Atlanta, Georgia
Print Name
Signature
Date
Phone Number
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION 12/2018 |
14 |
NOTICE OF CLAIM |
For injuries occurring on or after July 1, 2007, any claim filed with the Board for which neither medical nor income benefits have been paid shall stand dismissed with prejudice by operation of law if no hearing has been held within five years of the alleged date of injury. (O.C.G.A.
File Overview
| Fact | Description |
|---|---|
| Form Purpose | The WC-14 form is used to file a Notice of Claim, request a hearing, or request mediation with the Georgia State Board of Workers' Compensation. |
| Filing Requirements | Must be typed or printed in black ink, and a new form WC-14 must be completed to add an additional employer, insurer, or to add a date of injury. |
| False Statements Penalty | Knowingly providing false information on this form to obtain or deny workers’ compensation benefits can lead to civil and criminal penalties, including fines up to $10,000 per violation. |
| Dismissal of Claim | For injuries occurring on or after July 1, 2007, a claim will be dismissed with prejudice by operation of law if no hearing has been held within five years of the alleged date of injury, as per O.C.G.A. §34-9-100. |
Guide to Using Georgia Wc 14
Filling out the WC-14 form is a necessary step for individuals seeking to file a claim or request a hearing or mediation under the Georgia State Board of Workers' Compensation system. This form is pivotal in the initial stages of a claim, serving as formal notification of an incident and outlining the basis for any requested benefits or hearings. To ensure accuracy and compliance, it's critical to follow each step carefully, providing detailed and accurate information about the injury, the claimant, and the employer or insurer involved. After submission, the form will be reviewed by the State Board, and the claimant will be notified of the next steps in the process, including any additional documentation needed or scheduling of hearings.
- Check the appropriate box at the top to indicate whether you are filing a Notice of Claim Only, a Request for Hearing / Notice of Claim, or a Request for Mediation / Notice of Claim.
- Complete the section titled "A. CLAIM INFORMATION" with the employee's personal and injury details:
- Enter the employee's last name, first name, and middle initial.
- Fill in the date of injury, the employee's birthdate, and the county where the injury occurred.
- Provide the full mailing address of the employee, including city, state, and zip code.
- Input the employee's email address.
- In the "INSURER/EMPLOYER SELF-INSURER" section, add the relevant details:
- List the name and five-digit SBWC number of the employer or insurer.
- Include the mailing address, city, state, and zip code.
- Provide the employer or insurer's email address.
- For representation, enter the attorney's information under "ATTORNEY FOR EMPLOYEE/CLAIMANT" and "ATTORNEY FOR EMPLOYER/INSURER," if applicable:
- Include the attorney's name, mailing address, GA Bar Number, city, state, zip code, and email address.
- Detail the injury and claim information:
- Specify the part of the body injured.
- Enter the first date the employee was disabled due to the injury.
- If the claim involves a fatality, enter the date of death and provide claimants' information on additional sheets.
- Provide a brief description of the accident resulting in the injury.
- Select the issues for hearing or mediation in section "B. HEARING / MEDIATION ISSUES," checking the appropriate boxes and specifying other information as needed.
- In section "C. AFFIRMATION OF FILING PARTY," affirm that the information provided is true and correct to the best of your knowledge.
- Complete section "D. ENTRY OF APPEARANCE" if applicable, certifying the existence of a valid fee contract or Form WC-102B.
- Fill out the "E. CERTIFICATE OF SERVICE" section, certifying that copies of the form have been sent to all parties involved and to the State Board of Workers' Compensation.
- Finally, provide the name, signature, date, phone number, and email address of the person filing the claim at the bottom of the form.
After completing and submitting the WC-14 form, the claim will progress through the system. It's important to keep a copy of the form and any correspondence for personal records. The State Board of Workers' Compensation will guide the claimant through the next steps, which may involve additional documentation, a mediation process, or a hearing, depending on the specifics of the claim.
Obtain Clarifications on Georgia Wc 14
What is a Form WC-14 in Georgia?
Form WC-14, known as the Notice of Claim, is used in Georgia for individuals to either notify the State Board of Workers' Compensation about a work-related injury or illness, request a hearing regarding their workers' compensation claim, or request mediation. It's a way to officially start the process of claiming benefits for injuries or illnesses that occurred as a result of employment.
When should I use the Form WC-14?
You should use the Form WC-14 if you've been injured or have become ill due to your job and want to claim workers' compensation benefits. It can also be used to add an additional employer or insurer, or to update the date of injury. If more space is needed, attach additional sheets instead of altering the form. The form should be filled out and submitted as soon as possible after the injury or illness occurs.
How do I submit a Form WC-14?
The completed form must be typed or printed in black ink and submitted to the State Board of Workers' Compensation. You must also send a copy of this form to all involved parties, including employers and insurers. The submission address is provided in the form itself. Make sure to keep a copy for your records.
What are the different sections of the Form WC-14 and what do they mean?
- Notice of Claim Only: You're notifying the Board about your injury or illness.
- Request Hearing / Notice of Claim: You're notifying the Board and also requesting a hearing on your claim.
- Request for Mediation / Notice of Claim: You're seeking to resolve the claim through mediation.
The form also includes sections for claim information, issues for hearing or mediation, and an affirmation of the filing party ensuring all information provided is accurate.
What happens if I provide false information on the Form WC-14?
Providing false information on Form WC-14 for the purpose of obtaining or denying workers' compensation benefits is considered a crime. Such acts are subject to civil and criminal penalties, including fines of up to $10,000.00 per violation.
Can I add additional information if there is not enough space on the Form WC-14?
Yes, if you need extra space to provide additional details about the employer, insurer, or your injury, do not alter the form. Instead, attach additional sheets that include the necessary information.
Is there a deadline for submitting the Form WC-14?
While the form should be submitted as soon as possible after the injury or illness, specific deadlines may apply depending on your situation. For injuries occurring on or after July 1, 2007, any claim filed with the Board for which neither medical nor income benefits have been paid may be dismissed if no hearing has been held within five years of the alleged date of injury.
How do I know if I need to request a hearing or mediation?
You might consider requesting a hearing if you and your employer or their insurance company cannot agree on benefits. Mediation is an option for those looking to resolve disputes outside of a formal hearing, offering a potentially faster and less confrontational way to settle differences.
Who can help me fill out the Form WC-14?
While you can fill out the form yourself, you may seek assistance from a workers' compensation attorney, especially if you're planning to request a hearing or mediation. An attorney can provide guidance on how to fill out the form correctly and represent you during proceedings.
Common mistakes
Filling out the Georgia WC-14 form can be a straightforward process, but it's not uncommon for individuals to make mistakes. These errors can lead to delays or even affect the outcome of a claim. To help ensure accuracy and completeness, here is an expanded list of common mistakes people make when completing the Georgia WC-14 form:
**Not selecting the correct claim type** - The WC-14 form offers options to file a notice of claim only, request a hearing, or request mediation. It is crucial to check the appropriate box to accurately reflect the nature of your submission.
**Incomplete employer or insurer information** - Providing full and accurate details of the employer and insurer is necessary for the processing of the claim. This includes the name, mailing address, city, state, zip code, and email if available.
**Forgetting to add additional employers or insurers** - If there is more than one employer or insurer involved, a new Form WC-14 must be completed for each. Failing to do so can result in incomplete claim processing.
**Incorrect or incomplete claimant details** - Accurately filling out the claimant's personal information, such as name, birthdate, mailing address, and particularly the county of injury, is critical for proper filing and processing of the claim.
**Leaving out the date of injury** - The date of injury is a mandatory field that should be filled out with precision. If the injury resulted in death, the complete date of death must also be included.
**Not providing a detailed description of the accident and injury** - A clear and comprehensive description of the accident, including how it occurred and the type of injuries sustained, is essential for understanding the claim.
**Failure to list all benefits sought** - In the 'Hearing / Mediation Issues' section, it's important to accurately list and specify all the benefits you're seeking, including income benefits, medical benefits, and if applicable, penalties or attorney fees.
**Not completing the affirmation of filing party section** - This section confirms that all information provided on the form is true and correct. Skipping this affirmation can lead to issues with the claim's validity.
Beyond these specific items, there are several general tips to avoid mistakes:
Always use black ink or type for clarity and readability.
If additional space is needed, attach extra sheets instead of trying to alter the form itself.
Ensure that the form is signed and dated, as an unsigned form can lead to processing delays or be considered incomplete.
Before submitting, double-check all sections for accuracy and completeness to prevent unnecessary delays or complications.
By avoiding these common pitfalls, claimants can help ensure their WC-14 forms are processed smoothly and efficiently.
Documents used along the form
When navigating the workers' compensation claims process in Georgia, the WC-14 form serves as a crucial starting point. However, to facilitate a thorough understanding and handling of a case, various other documents might be utilized alongside this form. Here are five such forms and documents commonly encountered:
- WC-1 (Employer's First Report of Injury or Occupational Disease): This form is pivotal for recording an injury or disease that an employee suffers due to their job. Employers use it to report the incident to the Georgia State Board of Workers' Compensation.
- WC-2 (Notice of Payment or Suspension of Benefits): Employers or insurers submit this form to notify the Board and the employee of the initiation or change in payment of income benefits. It's essential for tracking the benefits paid to the injured worker.
- WC-3 (Notice to Controvert): When an employer or insurer disputes a claim, they file this form. It outlines the reasons for the denial of benefits, providing a pathway for contesting the claim.
- WC-104 (Employer’s Request for Hearing): If there’s a disagreement or need for adjustment regarding an employee's claim, employers use this form to request a hearing before the Board. It's a crucial step in resolving disputes.
- WC-108b (Change of Physician/Additional Treatment by Consent): This document allows for the change of a physician or additional treatment with the consensus of the employer/insurer and the employee. It ensures that the injured worker receives adequate medical care from a provider they trust.
Each of these forms plays a vital role in the workers' compensation process, complementing the WC-14 form to ensure that injured workers receive the benefits and care they are entitled to. By understanding and utilizing these documents effectively, all parties involved can navigate the complexities of workers' compensation with confidence and clarity.
Similar forms
The Georgia WC-14 Form is a multifaceted document used in workers' compensation cases to notify about a claim, request for a hearing, or mediation regarding an injury or accident that occurred during employment. This form plays a crucial role in the legal process related to workers' compensation. It is not unique in its purpose or function; there are several other documents in various legal contexts that share similarities with the Georgia WC-14 Form. Here are six documents that bear resemblance to the WC-14 Form in different legal scenarios:
SSA-827 (Authorization to Disclose Information to the Social Security Administration): Similar to the WC-14, this form is used to request and authorize the disclosure of information, but in the context of social security. Both forms involve the submission of personal and sensitive information to a governmental body to process claims related to either social security benefits or workers' compensation benefits.
VA Form 21-526EZ (Application for Disability Compensation and Related Compensation Benefits): This document, used by veterans to apply for disability benefits, shares similarities with the WC-14 in that it initiates a process for claiming benefits due to injury or illness. Both forms require detailed information about the nature of the injury or condition, although in different contexts.
Form I-485 (Application to Register Permanent Residence or Adjust Status): While primarily an immigration form, the I-485 shares the feature of initiating a critical process with substantial life implications, similar to the WC-14. Both documents necessitate accurate and comprehensive personal information to proceed with the application process.
FL-100 (Petition — Marriage/Domestic Partnership): Used to start the process of a divorce or legal separation in certain states, this form, like the WC-14, marks the beginning of a formal legal process. Both require specific personal and sensitive details about the parties involved, as well as the conditions pertinent to the claim or petition.
EEOC Charge of Discrimination Form: This is a document used to file a complaint of discrimination with the Equal Employment Opportunity Commission. Like the WC-14 Form, it serves as a notice to a regulatory body about a specific issue, requiring detailed information about the complainant, the defendant, and the nature of the complaint.
Form 1040 (U.S. Individual Income Tax Return): Although its purpose is for tax filing, the Form 1040 requires a comprehensive disclosure of personal and financial information to a government institution, similar to the WC-14's requirement for a detailed account of an injury and claim for benefits. Both play a foundational role in the processing of individual claims with respective government entities.
Each of these documents, while unique to its specific legal or administrative context, shares a commonality with the Georgia WC-14 Form in terms of initiating a complex process, requiring detailed personal information, and involving an interaction with a governmental or regulatory body to seek a certain type of relief or benefit.
Dos and Don'ts
When filling out the Georgia WC-14 form, a carefully structured approach ensures accuracy and compliance, crucial for the successful processing of your workers' compensation claim. Below are nine essential do's and don'ts to guide you through this process:
- Do ensure all information is typed or printed in black ink to maintain readability and adhere to submission standards.
- Do check the appropriate box at the top of the form to indicate whether you are filing a notice of claim only, requesting a hearing, or seeking mediation in addition to filing a notice of claim.
- Do provide complete and accurate information regarding your personal details, your employer, and the insurer or self-insurer to avoid delays.
- Do clearly describe the injury or illness, including the part of the body injured and a detailed account of how the injury or illness occurred.
- Do list all relevant dates, such as the date of injury, the first date of disability, and if applicable, the date of death, to ensure a comprehensive understanding of the timeline of events.
- Don't leave sections incomplete. If a section does not apply, mark it as "N/A" or "Not Applicable." Incomplete forms may lead to unnecessary delays or the outright rejection of the claim.
- Don't alter the form to add extra information or additional parties involved. Instead, attach additional sheets as needed, ensuring they are clearly marked and referenced on the main WC-14 form.
- Don't submit the form without verifying all information for accuracy. Incorrect or misrepresented details can lead to civil and criminal penalties.
- Don't forget to include the Certificate of Service section at the end of the form, certifying that you have sent a copy of the form to all relevant parties, including the State Board of Workers' Compensation.
Following these guidelines not only aids in the clear communication of your claim but also ensures adherence to the legal requirements set forth by the Georgia State Board of Workers' Compensation. Diligence and attention to detail throughout this process can significantly impact the outcome and efficiency of your claim's review.
Misconceptions
When navigating the intricacies of workers' compensation in Georgia, the Form WC-14, or Notice of Claim, emerges as a pivotal document. Despite its significance, several misconceptions swirl around its usage, implications, and requirements. Let's dissect four common myths and unveil the truths behind them.
- Myth 1: The WC-14 form is only for initiating a new claim.
Many people mistakenly believe that the Form WC-14 serves the sole purpose of initiating a new workers' compensation claim. However, this document's utility extends beyond just the initiation process. It is also crucial for requesting hearings or mediations related to an existing claim. Whether you're dealing with unresolved issues concerning benefits, disputes over the nature of the injury, or any adjustments to claim details, the WC-14 form facilitates these processes as well.
- Myth 2: Completing the WC-14 form automatically guarantees benefits.
Completing and submitting the WC-14 does not ensure that benefits will be automatically granted. This form merely starts the claim process or requests further action on a claim. After submission, the claim undergoes an evaluation process where evidence, such as medical reports and employment records, plays a crucial role in determining eligibility and the extent of benefits. Misunderstanding this can lead to unwarranted expectations from the claimants.
- Myth 3: Any alteration to the WC-14 form is acceptable if additional space is needed.
It's a common misconception that if more space is needed to provide information on the WC-14 form, alterations to the form itself are permissible. However, the correct procedure for including additional information is to attach separate sheets, without altering the original form. This ensures clarity and maintains the standardized format required by the Georgia State Board of Workers' Compensation.
- Myth 4: The WC-14 form is only necessary if legal representation is involved.
A prevalent falsehood is that the WC-14 form is only required when an attorney is engaged. The truth is, whether or not you have legal representation, this form is essential for initiating claims, requesting hearings, or seeking mediation. It's a critical step for anyone pursuing workers' compensation benefits, underscoring the form's importance in the workers' compensation claim process regardless of legal support.
Clarifying these misconceptions about the Form WC-14 illuminates the claim process's nuances within Georgia's workers' compensation landscape. It's crucial for employees and employers alike to grasp the form's true scope and function, ensuring that it's utilized correctly and effectively to facilitate claims and resolutions.
Key takeaways
Filling out and using the Georgia WC-14 form correctly is crucial for employees seeking workers' compensation benefits due to a workplace injury. Here are key takeaways to remember:
- Identify the Purpose: Determine whether you are filing for a Notice of Claim only, requesting a hearing, or requesting mediation in addition to the Notice of Claim. This choice is vital and must be clearly indicated on the form.
- Complete Information Required: Provide comprehensive and accurate information including the employee’s personal details, details of the injury such as the date and nature of the injury, and information about the employer and insurer.
- Additional Employer or Injury Dates: If there is a need to add another employer or a new date of injury, use a new Form WC-14. This ensures that all relevant parties are properly notified and involved in the claims process.
- Use Black Ink and Typed or Printed Text: For readability and to ensure the form is processed without delays, fill out the form in black ink and ensure it is either typed or clearly printed.
- Attach Additional Sheets if Necessary: If more space is needed to provide complete information, attach additional sheets instead of altering the form. This helps in keeping the documentation organized and accessible.
- Issues for Hearing/Mediation: Clearly list any issues such as Temporary Total Disability (TTD), Permanent Partial Disability (PPD), medical benefits, or other compensations being claimed. This helps in focusing the hearing or mediation on specific matters.
- Certify the Accuracy of Information: The person filling out the form must affirm that all information provided is true and accurate. Knowingly providing false information can lead to severe penalties, including fines.
- Certificate of Service: Ensure that a copy of the form is sent to all parties involved, including the State Board of Workers' Compensation. This is part of the certification process and is essential for the form's acceptance.
Understanding these key aspects can significantly aid in the smooth processing of a workers' compensation claim in Georgia through the WC-14 form. Attention to detail and adherence to instructions are critical throughout the process.
Popular PDF Forms
Ga Vaccine Exemption Form 2023 - Included in the form is a section for listing specific vaccines objected on religious grounds, including common ones such as Measles, Mumps, and Polio.
Georgia Advance Directive - Provides a legal avenue for people in Georgia to dictate their health care plans in moments of incapacity.
T 200 - The S200 form necessitates details of individuals responsible for directing and supervising the campaign, ensuring accountability in charitable solicitations.