Free Replacement Check Request Georgia Template in PDF
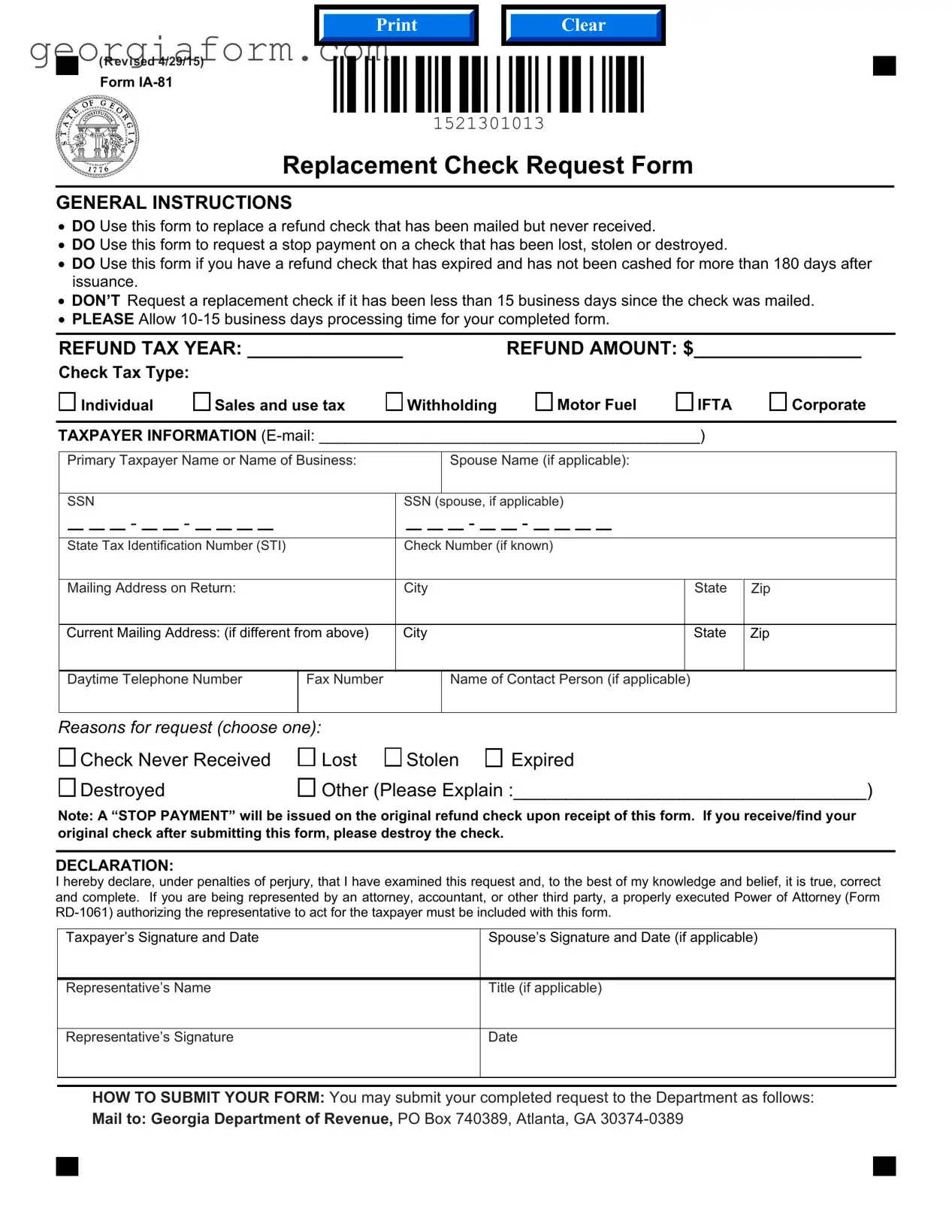
When individuals or businesses in Georgia encounter issues with refund checks that have been mailed but never received, lost, stolen, destroyed, or have expired without being cashed for more than 180 days, the Replacement Check Request Georgia Form IA-81 becomes a crucial tool for resolving these financial discrepancies. This form provides a structured pathway for requesting the replacement of such checks and is vital for ensuring that taxpayers can reclaim the funds rightfully owed to them by the state. It is essential, however, for applicants to wait at least 15 business days from the mailing date of the original check before requesting a replacement, and to allow a processing period of 10-15 business days for the completion of their request. The form requires detailed taxpayer information, including the tax year and amount of the refund, as well as a declaration of the reason for the request, such as a check never being received or a direct deposit failing to process. Furthermore, a declaration under the penalties of perjury confirms the truthfulness and accuracy of the information provided. For those represented by third parties, a Power of Attorney form must accompany the request. Once completed, the form can be submitted via mail or fax to the Georgia Department of Revenue, signalling the department to issue a stop payment on the original check and process the replacement. This carefully designed procedure safeguards both the state and the taxpayer, ensuring a cohesive and secure method for managing and rectifying these financial matters.
Form Sample
Clear
(R evised 4/29/15)
Form
Replacement Check Request Form
GENERAL INSTRUCTIONS
•DO Use this form to replace a refund check that has been mailed but never received.
•DO Use this form to request a stop payment on a check that has been lost, stolen or destroyed.
•DO Use this form if you have a refund check that has expired and has not been cashed for more than 180 days after issuance.
•DON’T Request a replacement check if it has been less than 15 business days since the check was mailed.
•PLEASE Allow
REFUND TAX YEAR: _____________ |
REFUND AMOUNT: $_______________ |
Check Tax Type:
Individual |
Sales and use tax |
Withholding |
Motor Fuel |
IFTA
Corporate
TAXPAYER INFORMATION
Primary Taxpayer Name or Name of Business: |
|
|
|
|
|
Spouse Name (if applicable): |
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SSN |
|
|
|
|
|
|
|
|
|
|
SSN |
(spouse, if applicable) |
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
- |
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State Tax Identification Number (STI) |
|
Check Number (if known) |
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address on Return: |
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
Zip |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
Current Mailing Address: (if different from above) |
City |
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
Zip |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
Daytime Telephone Number |
Fax Number |
|
|
|
|
|
Name of Contact Person (if applicable) |
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Reasons for request (choose one): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
Check Never Received |
Lost |
|
Stolen |
|
|
Expired |
|
|
|
||||||||||||||||||||||||||||||||
|
Destroyed |
|
|
|
|
|
|
|
|
|
Other (Please Explain :__________________________________) |
|||||||||||||||||||||||||||||||
Note: A “STOP PAYMENT” will be issued on the original refund check upon receipt of this form. If you receive/find your original check after submitting this form, please destroy the check.
DECLARATION:
I hereby declare, under penalties of perjury, that I have examined this request and, to the best of my knowledge and belief, it is true, correct and complete. If you are being represented by an attorney, accountant, or other third party, a properly executed Power of Attorney (Form
Taxpayer’s Signature and Date
Spouse’s Signature and Date (if applicable)
Representative’s Name
Title (if applicable)
Representative’s Signature
Date
HOW TO SUBMIT YOUR FORM: You may submit your completed request to the Department as follows:
Mail to: Georgia Department of Revenue, PO Box 740389, Atlanta, GA
File Overview
| Fact Name | Description |
|---|---|
| Purpose of the Form | This form is specifically designed for individuals or businesses seeking to replace a refund check that has either not been received, has been lost, stolen, destroyed, or has expired without being cashed for more than 180 days. |
| Eligibility to Request Replacement | Requesters must wait 15 business days since the original check was mailed before seeking a replacement. This ensures that there is sufficient time for the original check to be delivered. |
| Processing Time | After submitting the Replacement Check Request form, there is a processing period of 10-15 business days before the request can be completed and a replacement issued. |
| Governing Law | The process and issuance of the Replacement Check Request are governed by the laws and regulations of the Georgia Department of Revenue. This ensures a structured and legally compliant method to handle missing or expired checks. |
Guide to Using Replacement Check Request Georgia
If you're in the situation where a tax refund check from the Georgia Department of Revenue is lost, stolen, or maybe even expired, you'll want to know how to request a replacement check efficiently. The Replacement Check Request Form (Form IA-81) serves this purpose. For those who have waited over 15 business days since the check was supposedly mailed but have not received it, or find that their check cannot be cashed due to expiration (more than 180 days since issuance), this form is a lifeline. It's important to fill out this form carefully to ensure the processing of your request within the expected 10-15 business days.
- Identify the refund tax year and refund amount you're requesting the replacement check for, and specify the type of tax check you're replacing (e.g., Individual, Sales and use tax, etc.).
- Under TAXPAYER INFORMATION, provide your email address, the primary taxpayer's name or the name of the business, and the spouse's name if applicable. Also, include the Social Security Numbers (SSNs) or State Tax Identification Number (STIN), and the check number if known.
- Detail both the mailing address on the return and the current mailing address if they differ, to ensure the replacement check is sent to the correct location.
- Provide a daytime telephone number and a fax number, along with the name of a contact person if applicable, to facilitate communication.
- Select the reason for the replacement request (e.g., Check Never Received, Lost, Stolen, or Expired) and provide any necessary explanations in the space provided.
- Read and sign the declaration to affirm that the information provided is accurate and complete, understanding that this is under penalties of perjury. If you're filing jointly, ensure your spouse signs if applicable. Include the date next to each signature.
- If a third party represents you, include the representative’s name, title, and have them sign and date the form as well. Attach a properly executed Power of Attorney (Form RD-1061) if applicable.
- Once completed, you can submit your form to the Georgia Department of Revenue either by mail (to the address provided on the form) or via fax. The addresses and fax number are specified on the form for your convenience.
Following these steps will help streamline the process of obtaining a replacement check. Remember, the original check should not be cashed if it is found or received after submitting this request; it must be returned to the Department. Preparing your form with care and submitting it to the right place ensures that the replacement process is handled efficiently, getting you the refund you're entitled to without undue delay.
Obtain Clarifications on Replacement Check Request Georgia
What is the purpose of the Replacement Check Request Form IA-81 in Georgia?
This form is designed to be used by individuals who need a refund check to be reissued due to various reasons such as the check never having been received, being lost, stolen, destroyed, or a refund check that has expired (not been cashed) for more than 180 days after issuance. It also facilitates the request for a stop payment on the original check.
When should I not use the Replacement Check Request Form?
You should not request a replacement check if less than 15 business days have elapsed since the check was originally mailed. This period allows for any postal delays before considering the check as missing.
What is the processing time for a Replacement Check Request in Georgia?
After submitting the completed form, you should allow between 10 to 15 business days for the request to be processed.
What information is required on the form?
The form necessitates details such as the tax refund year, the amount of the refund, and the tax type (e.g., individual, corporate, sales and use tax). Additionally, taxpayer information including the name(s), Social Security Number(s) or State Tax Identification Number, contact details, and a thorough reason for the request need to be provided. If known, the check number should also be included.
What steps should I take if I find my original check after submitting a Replacement Check Request?
If you find or receive the original check after submitting the request, do not cash it. Instead, you are instructed to return the original check to the Department of Revenue immediately to avoid any financial discrepancies or legal issues.
Is there a declaration section in the form?
Yes, there is a declaration section at the end of the form. It requires the taxpayer (and spouse, if applicable) to sign, thereby declaring under penalty of perjury that the information provided is true, correct, and complete. If the taxpayer is being represented by a third party like an attorney or accountant, a properly executed Power of Attorney must also be submitted with the form.
How can I submit the completed Replacement Check Request Form?
The completed form can be submitted to the Georgia Department of Revenue either by mail or fax. The mailing address is 1800 Century Center Blvd NE, Suite 3104, Atlanta, GA 30345-3212, and the fax number is 404-417-4391.
Can I request a replacement check for any type of tax?
Yes, the form allows requests for various tax types including individual, corporate, sales and use tax, withholding, motor fuel, and International Fuel Tax Agreement (IFTA).
What should I do if I have not received a direct deposit?
If you expected a refund via direct deposit but did not receive it, this form also provides an option to report a direct deposit that was never received. It's important to verify your bank details and contact the Department for further instructions.
What is the importance of including a Power of Attorney with the form?
If a taxpayer is being represented by an attorney, accountant, or another third party, including a Power of Attorney is crucial. It legally authorizes the representative to act on behalf of the taxpayer regarding the refund check matter, ensuring that the request is handled appropriately and in accordance with the taxpayer’s wishes.
Common mistakes
When filling out the Replacement Check Request Georgia form, individuals often overlook or incorrectly handle key details that can significantly delay or complicate the process. Here are four common mistakes to avoid:
Not waiting the minimum period before requesting a replacement. The form explicitly states that a replacement check should not be requested if it has been less than 15 business days since the check was mailed. Initiating a request too early can lead to unnecessary processing delays and confusion.
Incorrect or incomplete taxpayer information. It is crucial to provide accurate and complete information regarding the taxpayer's name, Social Security Number (SSN) or State Tax Identification Number (STI), and current mailing address. Discrepancies or missing details in this section can lead to the rejection of the request or delays in processing.
Failing to choose a valid reason for the request or providing insufficient explanation for the 'Other' category. The form requires the requester to indicate why they are asking for a replacement check, such as the check never being received or being lost, stolen, expired, or destroyed. Selecting an inappropriate reason or not adequately explaining can result in processing delays.
Omitting the declaration signature and date. The declaration at the end of the form is a critical component that verifies the truthfulness and completeness of the information provided. Failure to sign or date this section can invalidate the request, as it is a declaration made under penalties of perjury.
To ensure a smooth and efficient processing experience, individuals should closely follow the form's instructions, provide all the required and accurate information, and ensure they have waited the appropriate amount of time since the check was initially mailed. By avoiding these common mistakes, the process of requesting a replacement check can be completed more swiftly and with fewer obstacles.
Documents used along the form
When dealing with the complexities of managing taxes and finances, ensuring you have all the necessary documents in order can significantly streamline any process. Particularly for residents of Georgia requesting a replacement check, the Replacement Check Request form plays a crucial role. However, this form often does not stand alone. Several other forms and documents are frequently used alongside it to provide comprehensive information and fulfill legal or procedural requirements.
- Form RD-1061 (Power of Attorney): Essential for authorizing a representative, like an attorney or accountant, to act on behalf of the taxpayer. It ensures that the designated individual can make requests, receive information, and make decisions regarding the taxpayer's financial matters.
- Form IT-511 (Income Tax Instructions): Offers detailed guidelines on filing individual income tax returns in Georgia, necessary for correctly submitting tax returns and understanding potential refund processes.
- Form 500 (Individual Income Tax Return): The primary form used for filing state income tax returns in Georgia. It's often associated with the replacement check request when discrepancies or questions about refunds arise.
- Form G-7 (Quarterly Return for Withholding Tax): Needed by employers or businesses that withhold Georgia state income tax from employees' wages. It may coincide with replacement check requests related to withholding tax refunds or adjustments.
- Form ST-5 (Sales Tax Certificate of Exemption): Useful for businesses involved in resale or exempt transactions. It may accompany replacement check requests when the issue pertains to sales and use tax refunds.
- Form 600 (Corporation Tax Return): Corporations filing taxes in Georgia might need a replacement check for their corporate tax refunds, making this form relevant to their proceedings.
- Form MV-1 (Motor Vehicle Title/Tag Application): While not directly related to tax refunds, individuals resolving issues with motor fuel tax refunds might also be dealing with vehicle registration or title concerns, requiring this form.
- Form T-8 (Affidavit of Non-receipt of Original Title): Similar to theReplacement Check Request, this form is used when an original vehicle title has not been received, often related to tax or fee payments made for vehicle registration.
- Bank Statement: Not a form, but often required to prove the non-receipt of a direct deposit refund. Providing a recent bank statement can support claims made with the Replacement Check Request form.
Altogether, these documents support and facilitate the processing of a replacement check request in Georgia, ensuring that all financial and legal bases are covered. Whether dealing with income, sales, corporate taxes, or other financial matters, having the right forms at hand can significantly ease the process of managing one's fiscal responsibilities.
Similar forms
Stop Payment Request: Similar to the Replacement Check Request form, a Stop Payment Request is used when a check issued has either been lost or stolen, or there are any errors on it that prevent cashing or deposit. Both forms initiate the process of stopping the financial transaction related to the original check and potentially issuing a new one.
Direct Deposit Enrollment Form: This form, similar in intent to parts of the Replacement Check Request, is used to set up direct deposit for various payments, such as refunds or regular payments. While the Replacement Check Request seeks to replace a mailed check, the Direct Deposit Enrollment Form seeks to avoid physical checks entirely, offering a more secure and direct method of receiving funds.
Refund Request Form: Used to request a refund for overpayment or erroneous charges, this form shares similarities with the Replacement Check Request form in terms of its use in rectifying financial discrepancies, such as an expired, lost, or incorrect refund check.
Lost or Stolen Credit Request Form: Though more commonly associated with credit cards, this form is similar to the Replacement Check Request in its function to report and mitigate the effects of lost or stolen financial instruments, allowing for the issuance of a replacement.
Claim for Damaged Currency: This form is used when currency is damaged or mutilated, requiring a replacement. Its function is parallel to the Replacement Check Request's objective of replacing non-negotiable or unusable financial documents with ones that can be properly utilized.
Declaration of Loss of Treasury Check: Employed to report and request replacement for Treasury checks that have been lost, stolen, or never received, this form closely mirrors the actions and purpose found within the Replacement Check Request by addressing issues with checks issued by the government.
Change of Address Form: Though its primary function is to update mailing information, this form can precede or accompany the Replacement Check Request in situations where checks are not received due to incorrect or outdated address information on file.
Affidavit of Forged Endorsement: This form is utilized when a check is wrongfully endorsed or cashed by another individual, similar to the Replacement Check Request's usage in cases of theft or loss. Both forms are used in the process of rectifying unauthorized or erroneous transactions.
Application for Duplicate or Paperless Title: Much like replacing a lost or destroyed check, this form is used to replace a vehicle title that has been lost, stolen, or damaged, embodying a similar concept of replacing essential documents for continued legal and financial dealings.
Power of Attorney (Form RD-1061): Mentioned in the Replacement Check Request instructions, a Power of Attorney form authorizes another party to act on someone's behalf in legal or financial matters. Its connection to the Replacement Check Request form underlines the importance of proper representation in handling sensitive financial transactions.
Dos and Don'ts
When dealing with the process of requesting a replacement check in Georgia, it's crucial to follow specific guidelines to ensure the process is handled efficiently and accurately. Here are lists of what you should and shouldn't do when filling out the Replacement Check Request Georgia form.
Things You Should Do
- Use the form to replace a refund check that was mailed but never received, to request a stop payment on a check that has been lost, stolen, or destroyed, or if you have a refund check that expired and has not been cashed for more than 180 days after issuance.
- Ensure you have allowed for a waiting period of at least 15 business days after the check was initially mailed before requesting a replacement. This provides enough time to mitigate any postal service delays.
- Accurately fill out all required taxpayer information, including the primary taxpayer name or name of the business, SSN or State Tax Identification Number (STI), mailing addresses, and contact numbers.
- Include a declaration at the end of the form, signed under the penalties of perjury, affirming that the information provided is true, correct, and complete. If a third party represents you, ensure to attach a properly executed Power of Attorney (Form RD-1061).
Things You Shouldn't Do
- Do not request a replacement check if it has been less than 15 business days since the check was originally mailed. This timeframe accounts for potential postal service delays.
- Avoid cashing the original check if you find it after submitting this form for a replacement. You must return the original check to the Department to prevent legal issues.
- Do not leave any sections of the form blank, especially those related to the reason for the replacement request (e.g., lost, stolen, destroyed, expired), to avoid delays in processing.
- Refrain from submitting incomplete forms or lacking the necessary attachments, such as the declaration and Power of Attorney (if a third party represents you), as this can result in processing delays.
Adhering to these do's and don'ts can significantly ease the process of requesting a replacement check, ensuring you receive your due funds timely and efficiently.
Misconceptions
When dealing with the process of replacing a lost, stolen, or expired check in Georgia, it's easy to stumble upon misconceptions. Here are ten common misunderstandings about the Replacement Check Request Georgia form, clarified to help you navigate your way with confidence:
- Everyone can use this form for any type of missing payment. This form is specifically designed for replacing refund checks related to taxes. It's not applicable for other types of state-issued payments.
- You should wait indefinitely for the original check before requesting a replacement. The form advises waiting no less than 15 business days since the check was mailed, but there's no need to wait beyond this period.
- A replacement check is instantly processed. Processing time for a completed form is 10-15 business days. Patience is key.
- The form is only for individuals. Both businesses and individuals can use the form, provided it's related to tax refund checks.
- Submitting the form guarantees immediate stop payment on the original check. While a stop payment is issued upon receipt of the form, it may take time for this to be fully processed.
- Once you've submitted the form, you can cash the original check if it arrives. If the original check arrives after you've submitted the form, you must not cash it. Instead, return it to the Department as instructed.
- Only the primary taxpayer needs to sign the form. If applicable, both the primary taxpayer and their spouse must sign the replacement request form.
- You must know the check number to complete the form. While helpful, the check number is not required to submit a request. You can still submit a request without it.
- Electronic submission is an option for everyone. The preferred submission methods are via mail or fax. Make sure you check the latest guidance in case this changes.
- Any form of contact information is acceptable. The form requires specific contact details, including a daytime phone number and, if applicable, a fax number and email. Providing accurate and complete contact information is crucial.
Understanding these aspects of the Replacement Check Request Georgia form can prevent unnecessary delays and ensure your request is handled smoothly. Remember, the goal is to aid you in receiving your rightfully owed funds in a timely and secure manner.
Key takeaways
When dealing with lost, stolen, or expired refund checks in Georgia, the Replacement Check Request Form IA-81 comes into play. It offers a structured process for requesting a new check under various circumstances. Here are five key points to understand when filling out and using this form:
- Eligibility for Request: This form is specifically for use when a refund check was not received, has been lost, stolen, destroyed, or has expired without being cashed for over 180 days. Importantly, if the original check was mailed out less than 15 business days ago, a replacement request should not be made yet.
- Processing Time: After submitting the form, it’s essential to allow 10-15 business days for the request to be processed. This time frame is crucial for planning and setting expectations regarding the arrival of the replacement check.
- Detailed Information Required: Filling out the form requires specific taxpayer information, including the tax year of the refund, the amount, type of tax, and personal identification details. A detailed and accurate completion of the form ensures a smoother processing of the request.
- Multiple Tax Types Covered: Whether the refund is for individual income tax, sales and use tax, withholding, motor fuel, IFTA, or corporate tax, the form accommodates various tax types. This versatility means that individuals and businesses alike can use it for their specific needs.
- Important Steps After Submission: A critical instruction is that if the original check surfaces after submitting the replacement request, it should not be cashed. The correct action is to return the original check to the Department. Furthermore, if a taxpayer is represented by a third party, a Power of Attorney form must be included with the submission, ensuring that all legal bases are covered.
Understanding and adhering to these guidelines when interacting with the Replacement Check Request Form can significantly streamline the process of rectifying issues with refund checks in Georgia. Whether it's the waiting period, the required information, or the steps after an original check is found, each element contributes to a more efficient resolution of replacement check requests.
Popular PDF Forms
What Can You Do to Extend Time Before Car Is Towed Ga - The form serves as a legal declaration from repair facilities about the abandonment status of a vehicle, in line with Georgia's regulations.
Georgia Depreciation Rules - Applicants must specify if the loss is being carried forward to future tax years.