Free Wc 200A Georgia Template in PDF
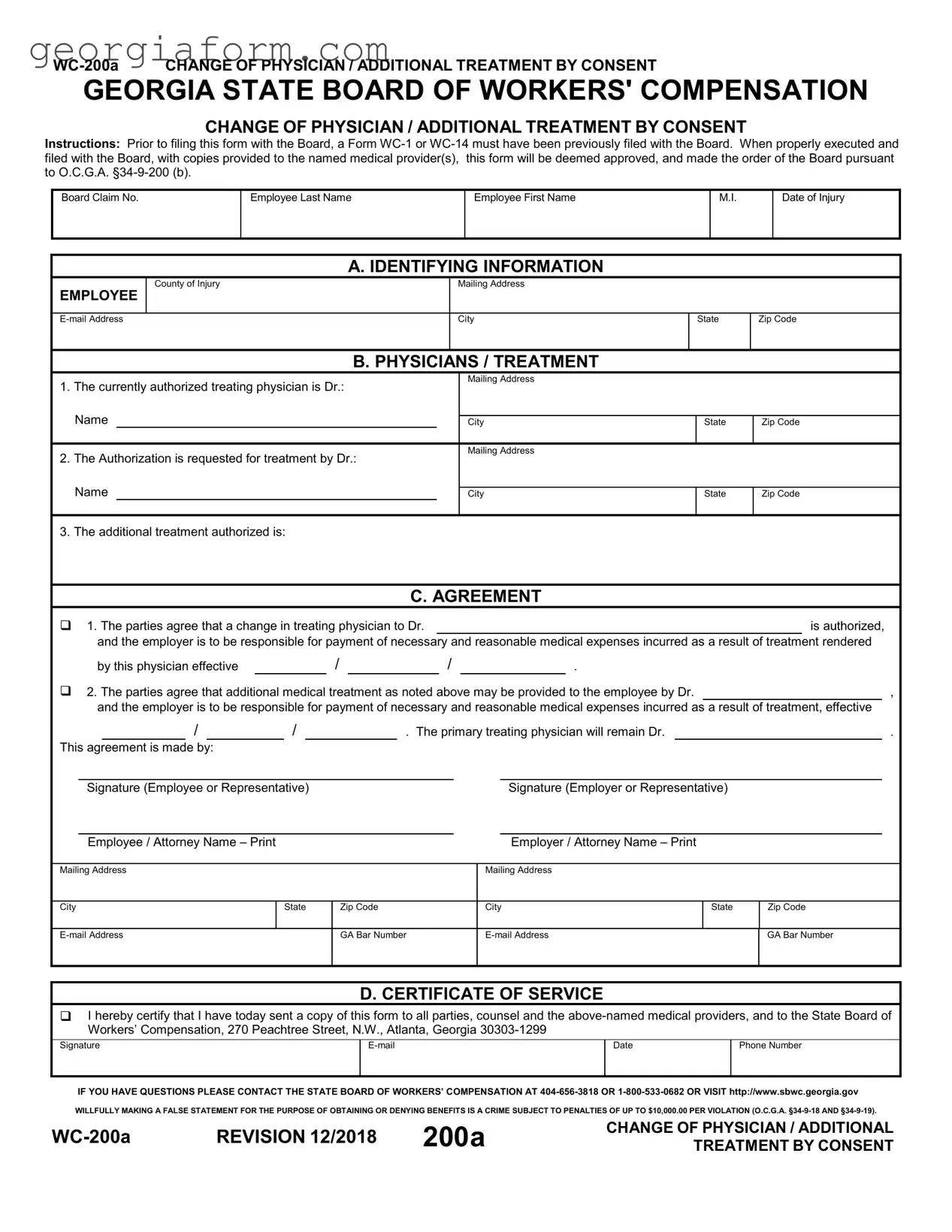
The WC-200a form plays a pivotal role in the Georgia State Board of Workers’ Compensation system, offering a structured process for employees seeking a change in their authorized treating physician or aiming to obtain additional treatment by consent after a workplace injury. This document serves as a formal request, requiring detailed information about the employee, the initially authorized treating physician, and the new medical provider proposed by the employee or the employer. Prior to the submission of the WC-200a form, either a WC-1 or WC-14 must already be on file with the Board, establishing the foundation for this subsequent request. By correctly completing and filing this form, and ensuring copies are delivered to the relevant medical providers, the request becomes effective immediately upon filing, presuming it adheres to the guidelines set forth under O.C.G.A. §34-9-200(b). It encompasses sections for identifying information about the employee, details of the currently authorized and newly requested physicians, an explicit agreement section outlining the consent from both parties for the change or addition in medical treatment, and a certificate of service verifying that all concerned parties, including the State Board of Workers' Compensation, have been duly notified. This form embodies a vital procedural step, ensuring that employees have the means to seek necessary and reasonable medical attention, with the assurance of financial responsibility from the employer for such treatment, all within the legal framework provided by the state of Georgia.
Form Sample
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
CHANGE OF PHYSICIAN / ADDITIONAL TREATMENT BY CONSENT
Instructions: Prior to filing this form with the Board, a Form
Board Claim No.
Employee Last Name
Employee First Name
M.I.
Date of Injury
A. IDENTIFYING INFORMATION
EMPLOYEE
County of Injury
Mailing Address
City
State
Zip Code
B. PHYSICIANS / TREATMENT
1.The currently authorized treating physician is Dr.:  Name
Name
2.The Authorization is requested for treatment by Dr.:
Mailing Address
City
Mailing Address
State
Zip Code
Name
City
State
Zip Code
3. The additional treatment authorized is:
C. AGREEMENT
1. The parties agree that a change in treating physician to Dr. |
|
|
|
|
|
|
|
|
is authorized, |
||||||||||||||||
|
and the employer is to be responsible for payment of necessary and reasonable medical expenses incurred as a result of treatment rendered |
||||||||||||||||||||||||
|
by this physician effective |
|
|
|
/ |
|
|
/ |
|
|
. |
|
|
|
|
|
|||||||||
2. The parties agree that additional medical treatment as noted above may be provided to the employee by Dr. |
|
|
, |
||||||||||||||||||||||
|
and the employer is to be responsible for payment of necessary and reasonable medical expenses incurred as a result of treatment, effective |
||||||||||||||||||||||||
|
|
/ |
|
|
|
/ |
|
|
|
|
|
. The primary treating physician will remain Dr. |
|
|
|
. |
|||||||||
This agreement is made by: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Signature (Employee or Representative) |
|
|
|
|
|
|
|
|
|
|
Signature (Employer or Representative) |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Employee / Attorney Name – Print |
|
|
|
|
|
|
|
|
|
|
|
|
Employer / Attorney Name – Print |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
City |
|
State |
|
|
Zip Code |
|
City |
State |
Zip Code |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
GA Bar Number |
|
|
GA Bar Number |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all parties, counsel and the
Signature |
Date |
Phone Number |
|
|
|
|
|
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION 12/2018 |
200a |
CHANGE OF PHYSICIAN / ADDITIONAL |
|
TREATMENT BY CONSENT |
File Overview
| Fact Name | Description |
|---|---|
| Form Purpose | The WC-200a form is used to request a change of physician or additional treatment by consent in Georgia workers' compensation cases. |
| Governing Law | This form is governed by O.C.G.A. §34-9-200(b), which addresses changes in medical care providers and additional treatment in workers' compensation cases. |
| Prerequisite Filing | A Form WC-1 or WC-14 must have been previously filed with the Board before submitting the WC-200a. |
| Approval Process | When properly executed and filed with the Board, and with copies provided to the medical provider(s), the form is deemed approved and becomes an order of the Board. |
| Section A - Identifying Information | Section A collects the employee's identifying information, including name, address, and date of injury. |
| Section B - Physicians / Treatment | Section B records the details about the currently authorized treating physician and the requested new physician or additional treatment. |
| Section C - Agreement | This section contains the agreement between the parties regarding the change of physician or authorization of additional treatment, including responsibility for payment. |
| Penalties for False Statements | Making a false statement for the purpose of obtaining or denying benefits is a crime with penalties up to $10,000.00 per violation as per O.C.G.A. §34-9-18 and §34-9-19. |
| Certificate of Service | A certificate of service section is included for certifying that copies of the form have been sent to all relevant parties. |
| Contact Information | The form provides contact information for the State Board of Workers' Compensation for further assistance. |
| Form Revision Date | The last revision of the WC-200a form was in December 2018. |
Guide to Using Wc 200A Georgia
After experiencing an injury at work, it may become necessary to adjust your medical care by changing your treating physician or seeking additional treatment. This is where the WC-200a form comes into play for Georgia residents. Completing and filing this document correctly ensures that the transition or addition in care is recognized and approved by the Georgia State Board of Workers' Compensation. Following a clear step-by-step process will guide you through filling out this form with precision, helping facilitate a smooth transition in your medical treatment and support a continued path toward recovery.
- Ensure a Form WC-1 or WC-14 has been previously filed with the Board. This is a crucial prerequisite before filling out the WC-200a.
- Start with Section A: Identifying Information. Enter the employee's last name, first name, and middle initial. Fill in the date of injury, county of injury, and the employee's complete mailing address including city, state, and zip code. Don't forget the employee's email address for communication.
- In Section B: Physicians / Treatment, indicate the current authorized treating physician's name and address. Then, for the physician you wish to change to or for the additional treatment needed, provide the new doctor's name and address. Specify the type of additional treatment requested if applicable.
- Move to Section C: Agreement. Choose the appropriate box to indicate whether this form is being used for a change of treating physician or for requesting additional treatment. Fill in the effective date of this change or additional treatment.
- Both the employee (or their representative) and the employer (or their representative) must sign and print their names, providing their mailing addresses, city, state, zip code, email addresses, and GA Bar Number if applicable.
- Finally, in Section D: Certificate of Service, certify that a copy of this form has been sent to all involved parties, including the State Board of Workers’ Compensation. Include your signature, email, phone number, and the date.
Upon correctly completing and submitting the WC-200a form, along with any required supporting documentation, your request for a change of physician or additional treatment will be processed. It's essential to provide copies to all named medical providers and adhere to any additional instructions from the Georgia State Board of Workers’ Compensation to ensure your medical care adjustments are recognized and enacted without delay.
Obtain Clarifications on Wc 200A Georgia
What is the WC-200a form used for in Georgia?
The WC-200a form is utilized to request a change of physician or to seek consent for additional medical treatment under the Georgia State Board of Workers' Compensation guidelines. It serves as a formal request to the Board and, when properly executed and filed, allows for the alteration in medical care or additional treatments as specified in the agreement sections of the form.
When should the WC-200a form be filed?
This form should be filed after a Form WC-1 (Notice of Injury or Occupational Disease) or WC-14 (Notice of Claim/Request for Hearing/Request for Mediation) has already been submitted to the Georgia State Board of Workers' Compensation. It specifically addresses changes or additions to medical treatment and should be filed whenever such modifications are needed and agreed upon.
Who needs to sign the WC-200a form?
Both the employee (or their representative) and the employer (or their representative) must sign the WC-200a form to acknowledge their agreement on the change of physician or additional treatment. These signatures are crucial for the form to be approved and processed by the State Board of Workers' Compensation.
What information is required on the WC-200a form?
The form requires detailed information including, but not limited to, the employee’s identifying information, details of the current and requested medical providers, and specific treatment or physician change requests. Additionally, mailing addresses, and contact information for both parties’ representatives are required, alongside signatures to validate the agreement.
How is the WC-200a form submitted?
After completing the form and obtaining the necessary signatures, it must be filed with the Georgia State Board of Workers' Compensation. Copies should also be provided to the newly named medical provider(s) and all involved parties, ensuring full acknowledgment and compliance with the agreed upon changes or additions in treatment.
What happens after the WC-200a form is filed?
Once properly executed and filed, the form is deemed approved and becomes the order of the Board, as per the Official Code of Georgia Annotated (O.C.G.A.) §34-9-200 (b). This means the requested change of physician or additional treatment is authorized, with the employer responsible for the payment of necessary and reasonable medical expenses incurred due to this change or additional treatment.
Is there a deadline for filing the WC-200a form?
The form must be filed promptly following the agreement between the employee and employer regarding the change of physician or additional medical treatment. Although no specific deadline is mentioned, timely submission is essential to ensure that the employee receives the necessary medical care without undue delay.
What should you do if the parties disagree on the contents of the WC-200a form?
If there is disagreement on the change of physician or additional treatment outlined in the WC-200a form, the parties may seek mediation or potentially a hearing with the Georgia State Board of Workers' Compensation to resolve the dispute. Legal counsel may be advisable in these circumstances to protect the rights and interests of the involved parties.
Can the WC-200a form be altered after it has been filed?
Once approved, changes to the agreed upon medical treatment or physician must be requested through a new WC-200a form submission, outlining the new changes and again requiring agreement and signatures from both parties. The process mirrors the initial submission and seeks to ensure all parties are in agreement with the medical care provided.
What penalties exist for falsifying information on the WC-200a form?
Willfully making a false statement on the WC-200a form for the purpose of obtaining or denying benefits is a crime that can lead to penalties of up to $10,000.00 per violation, as outlined in O.C.G.A. §34-9-18 and §34-9-19. It is critical that all information provided on the form is accurate and truthful to avoid legal repercussions.
Common mistakes
Not verifying pre-existing documentation: Filling out a WC-200a form without having previously filed a WC-1 or WC-14 form with the Georgia State Board of Workers' Compensation is a common mistake. These forms are prerequisites and confirm an existing claim, ensuring the process aligns with the legal requirements outlined under O.C.G.A. §34-9-200 (b).
Incorrect or incomplete physician information: Another mistake involves inaccurately listing the authorized treating physician or the new physician to which treatment is being transferred or added. It is essential to provide the full name and complete contact details of both physicians to avoid delays or disputes regarding the authorization for a change in treating physician or additional treatment consent.
Failing to specify treatment details: Omitting the specifics of the additional treatment authorized can lead to misunderstandings about what medical care the employer is responsible for financing. Clearly stating the type of additional treatment helps in ensuring that necessary and reasonable medical expenses are covered effective from the date mentioned.
Inadequate agreement documentation: Not properly executing the agreement section can significantly impact the validity of the request. It's imperative that the agreement specifies whether it's a change in treating physician or additional medical treatment is being allowed, and both the employee (or representative) and employer (or representative) must provide their signatures to validate the consent.
Improper certificate of service: Neglecting to certify that copies of the form have been sent to all relevant parties, including the State Board of Workers' Compensation, is a critical oversight. This certification, which must include the sender's signature, date, email, and phone number, ensures that the document is legally served and all parties are informed, keeping the process transparent.
While these mistakes may seem minor, they can significantly impact the outcome and efficiency of processing the WC-200a form. It is crucial to approach this documentation with careful attention to detail, verifying all information for accuracy and completeness to ensure that the change of physician or additional treatment by consent is executed smoothly and within legal parameters.
Documents used along the form
When navigating through the realm of workers' compensation in Georgia, understanding the paperwork involved is crucial for employees seeking medical treatment or a change in physician due to a workplace injury. The WC-200a form plays a central role in facilitating these requests. However, this document is often just one piece in a puzzle of necessary forms that ensure a smooth process and proper communication between all parties involved. Let's explore some of the other essential forms and documents commonly used alongside the WC-200a form.
- WC-1 (Notice of Injury or Occupational Disease): This form serves as the initial report of work-related injury or illness. It is crucial for starting the claim process, detailing the specifics of the injury and the circumstances under which it occurred.
- WC-14 (Notice of Claim): When an employee seeks to initiate a workers' compensation claim, this form is filed with the Georgia State Board of Workers' Compensation. It officially notifies the Board, the employer, and the insurance carrier of the intent to pursue workers' compensation benefits.
- WC-104 (Notice to Employee of Medical Release to Return to Work with Restrictions or Limitations): When a physician releases an employee to return to work with specific restrictions or limitations, this form is used to communicate those conditions clearly to all parties, ensuring the employee's health is not compromised upon their return to the workplace.
- WC-108b (Employer’s Request for WC-240 & Suspension of Benefits or Notification of Refusal of Suitable Employment Offered Under O.C.G.A. §34-9-240): This form is used by the employer to either request authorization to suspend benefits due to an offer of suitable employment that the employee refused or to proceed with a designated examination under O.C.G.A. §34-9-240.
- WC-205 (Request for Authorization of Treatment or Testing by Authorized Medical Provider): Medical providers use this form to request pre-authorization for specific treatments or tests from the employer or insurer, ensuring that the proposed care or diagnostics is approved and covered under workers' compensation.
- WC-207 (Authorization and Consent to Release Information): This form is used by employees to authorize the release of medical, employment, or other relevant information to their employers, insurance carriers, or legal representatives, facilitating the smooth exchange of necessary details for processing a claim.
Understanding these forms and their appropriate contexts is vital for any employee navigating the workers' compensation system in Georgia. Each document plays a specific role in ensuring the process is transparent, efficient, and fair for all parties involved. Whether you're filing for a change in physician, seeking authorization for additional treatment, or reporting an injury, knowledge of these forms empowers you to advocate for your rights and facilitates a smoother journey to recovery.
Similar forms
The WC-1 First Report of Injury form in Georgia is similar because it initiates the workers' compensation claim process, just as the WC-200a form is involved in the continuation of treatment under that claim. The WC-1 form is where it all starts, requiring detailed information about the injury, while the WC-200a involves modification regarding the medical treatment.
The WC-14 Notice of Claim form is also closely related, as it must be filed with the Board prior to the WC-200a. It notifies the board of the worker’s intent to seek compensation, setting the groundwork for actions like changing physicians or receiving additional treatment as outlined in the WC-200a form.
The WC-104 Employer’s Request for Suspension of Benefits shares a connection in that it addresses changes in the worker’s compensation case status, similar to how the WC-200a form might bring about changes due to a switch in medical providers or additional treatments.
The IPB-1 Panel of Physicians form is related because, like the WC-200a, it involves the selection of medical providers. The key difference is that the IPB-1 is about establishing the initial panel of physicians, while the WC-200a may change or add to the list of approved practitioners.
The WC-PMT Payment of Medical Benefits form intersects with the WC-200a through the aspect of medical expenses. The WC-PMT deals with the payment for medical services, closely aligning with the WC-200a's discussions around the responsibility for newly authorized medical treatments.
The WC-240 Return to Work with Restrictions form is relevant since changes or additions in treatment via the WC-200a could affect an employee's ability to return to work, similar to what is detailed in a WC-240, which outlines an employee’s return to work under specific restrictions.
The WC-R1 Request for Rehabilitation shares a theme with the WC-200a regarding the continuation or change in medical care, focusing specifically on rehabilitation services. Both forms contribute to the discussion and documentation of ongoing treatment necessary for the employee’s recovery.
The WC-207 Authorization to Release Information is linked with the WC-200a process, as it involves the sharing of medical information between providers, employers, and the state board. Both documents are vital for maintaining transparency and communication regarding treatment and workplace injuries.
A Settlement Agreement form overlaps with the intent behind the WC-200a because both may conclude specific aspects of a case, whether it be finalizing treatment arrangements or settling claims. The WC-200a's agreements about treatment changes or additions can be precedents to eventual settlements.
Last is the MG-2 Request for Approval of Variance form, which is found in other states like New York. It’s similar to the WC-200a as both forms are geared towards altering the course of an employee's medical treatment by gaining consent for variations from the standard treatment protocols or, in Georgia’s case, changing the physician.
Dos and Don'ts
When completing the WC-200a Georgia form, which is utilized for changes in physician or additional treatments by consent in a workers' compensation claim, certain practices should be followed to ensure the form is correctly filled out and processed efficiently. Here are ten important dos and don'ts:
- Do ensure that either a Form WC-1 or WC-14 has been filed with the Board before submitting the WC-200a form, as required.
- Do accurately fill in all requested identifying information for the employee, including the last name, first name, middle initial, date of injury, mailing address, county of injury, and email address.
- Do clearly list the currently authorized treating physician and the new physician being requested for a change of treatment or additional treatment, including their full names and addresses.
- Do specify the type of additional treatment being requested in the relevant section of the form to avoid any ambiguity or delay in processing.
- Do check the appropriate agreement box that accurately reflects the request being made, whether it's a change of treating physician or approval for additional medical treatment.
- Don't leave any sections blank. If a section does not apply, fill in "N/A" to indicate this status.
- Don't forget to provide signatures from both the employee (or representative) and the employer (or representative) to validate the agreement as outlined on the form.
- Don't send the form to the State Board of Workers' Compensation without first ensuring that copies have been sent to all required parties, including the named medical providers.
- Don't neglect the Certificate of Service section at the end of the form; this is crucial for documenting that all parties have been notified as required.
- Don't make false statements on the form. Be reminded that willfully making a false statement for the purpose of obtaining or denying benefits is a crime with significant penalties.
By adhering to these guidelines, the process of changing physicians or requesting additional treatment under the workers' compensation system in Georgia can be made smoother and more efficient for all parties involved.
Misconceptions
Understanding the WC-200a form in Georgia can be confusing at first glance. This document plays a critical role in the workers' compensation system, specifically when a change of physician is required or when additional treatment is sought. It's essential to clear up several common misconceptions surrounding this form to ensure that employees and employers alike navigate their rights and responsibilities with clarity.
- Misconception 1: The WC-200a Form Is Optional in Changing Physicians
Many believe that to change a treating physician or to seek additional medical treatment, an informal agreement between the employee and employer is enough. However, the WC-200a form is a mandatory document that needs to be properly executed and filed with the Georgia State Board of Workers' Compensation. Any change in the treatment plan or physician without this form, duly processed, is not legally binding.
- Misconception 2: Approval from the State Board Is Always Required
While it might seem that every change or addition in treatment necessitates prior approval from the State Board of Workers' Compensation, the reality is slightly different. Once the WC-200a form is correctly filled out, signed by the necessary parties, and filed with the Board (with copies appropriately distributed), the agreement is automatically deemed approved, as per O.C.G.A. §34-9-200 (b). Explicit approval from the Board is not needed unless the form is contested.
- Misconception 3: Filing a WC-200a Is the First Step in the Claims Process
A critical misunderstanding is that the submission of a WC-200a form can initiate a workers' compensation claim. In truth, either a Form WC-1, reporting an injury or occupational disease, or a WC-14, filing a claim for compensation, must have already been filed with the Board. The WC-200a serves a specific function in the ongoing management of a claim, particularly concerning medical treatment, rather than starting it.
- Misconception 4: The Form Can Be Filed Without Employee or Employer Agreement
It's often misconceived that a WC-200a form can proceed through the workers' compensation system without explicit consent from all parties involved. However, this form requires agreement and signatures from both the employee (or their representative) and the employer (or their representative) for a change of physician or additional treatment. Without these agreements in place, the request outlined in the form cannot be enacted.
Understanding these nuances is critical for everyone involved in the workers' compensation system. Whether you're an employee undergoing treatment or an employer managing a claim, knowing how to correctly utilize the WC-200a form not only streamlines the process but also ensures that all legal requirements are met.
Key takeaways
The WC-200A form plays a critical role in the workers' compensation process in Georgia. It is essential for employees, employers, and attorneys to understand the intricacies of its use to ensure the smooth continuation of medical treatment and adherence to legal requirements. Here are key takeaways regarding the completion and application of the WC-200A form:
- Before the WC-200A form can be filed with the Georgia State Board of Workers' Compensation, a Form WC-1 or WC-14 must have been previously filed. This ensures that there is an existing claim within the system.
- The form allows for a change in the authorized treating physician or the addition of medical treatment by mutual consent of the involved parties.
- To effect a change of physician or authorize additional treatment, the form must be accurately completed and submitted to the Board. Upon proper execution and submission, the form is deemed approved and considered an order of the Board.
- Full and precise identification details of the employee, including their name, mailing address, and county of injury, are crucial for the processing of the form.
- Details of both the current authorized treating physician and the newly requested physician or additional treatment must be clearly provided to avoid any confusion or delay.
- Consent is explicitly required for either changing the treating physician or for additional treatment. This necessitates the agreement of the parties involved, with the employer responsible for the payment of necessary and reasonable medical expenses incurred from the treatment.
- Signatures from both the employee (or their representative) and the employer (or their representative) are mandatory for the validity of the agreement.
- A Certificate of Service section requires the person filing the form to certify that a copy has been provided to all relevant parties, including the medical providers, counsel, and the State Board of Workers' Compensation itself.
- Contact information for the State Board of Workers' Compensation is provided for individuals who may have questions or require further assistance regarding the form or its implications.
Completing the WC-200A form correctly is vital for ensuring that employees receive the necessary medical care in a timely manner while also meeting the legal obligations outlined by the Georgia State Board of Workers' Compensation. This process, grounded in mutual consent, facilitates smoother transitions in care and helps maintain the integrity of workers' compensation claims.
Popular PDF Forms
Georgia Workers Compensation Forms - It helps in defining the scope of work an injured employee can undertake, facilitating smoother transitions back into the workforce.
Can You Be Adopted at 18 - Chart your course to a finalized family bond with the Georgia Adult Adoption Petition form, your map to adoption success.